

Binodal, wireless epidermal electronic systems with in-sensor analytics for neonatal intensive care
- PMID: 30819934
- PMCID: PMC6510306
- DOI: 10.1126/science.aau0780
Binodal, wireless epidermal electronic systems with in-sensor analytics for neonatal intensive care
Abstract
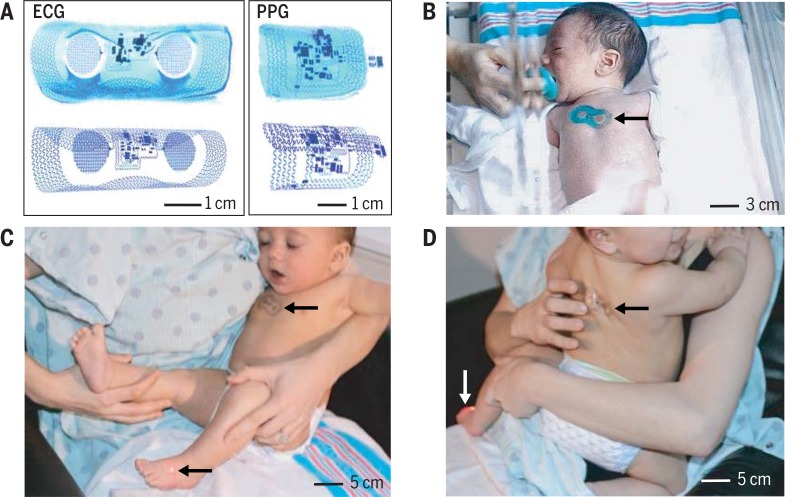
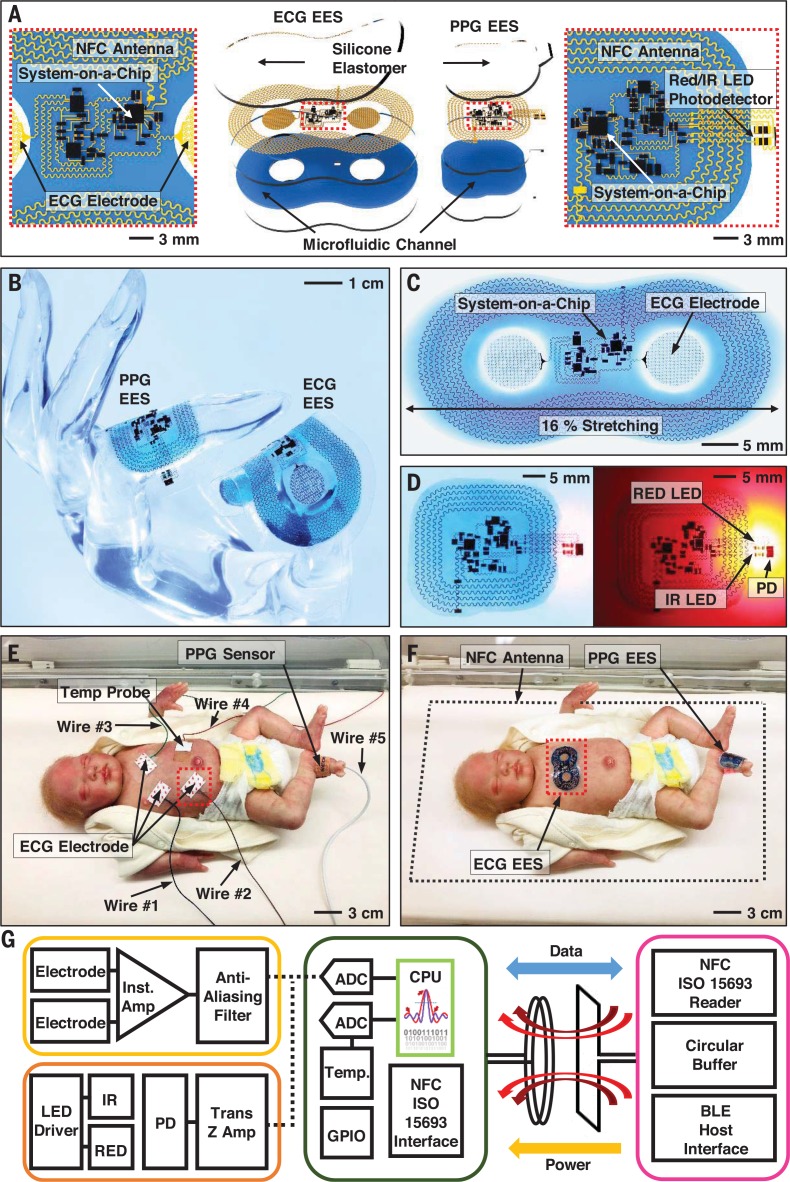
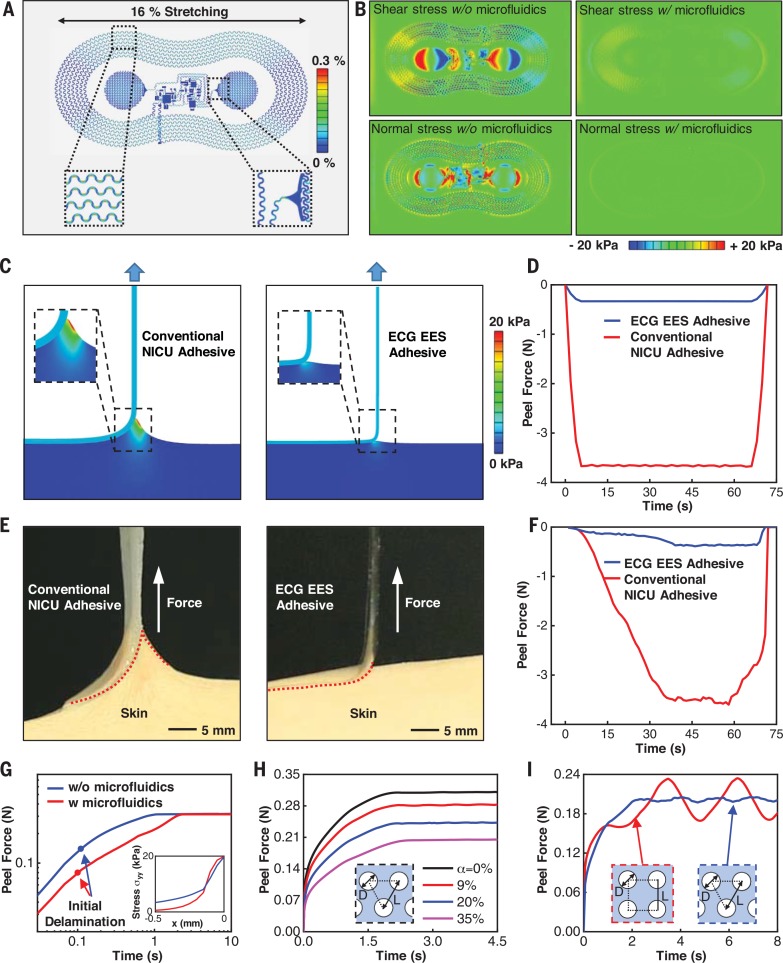
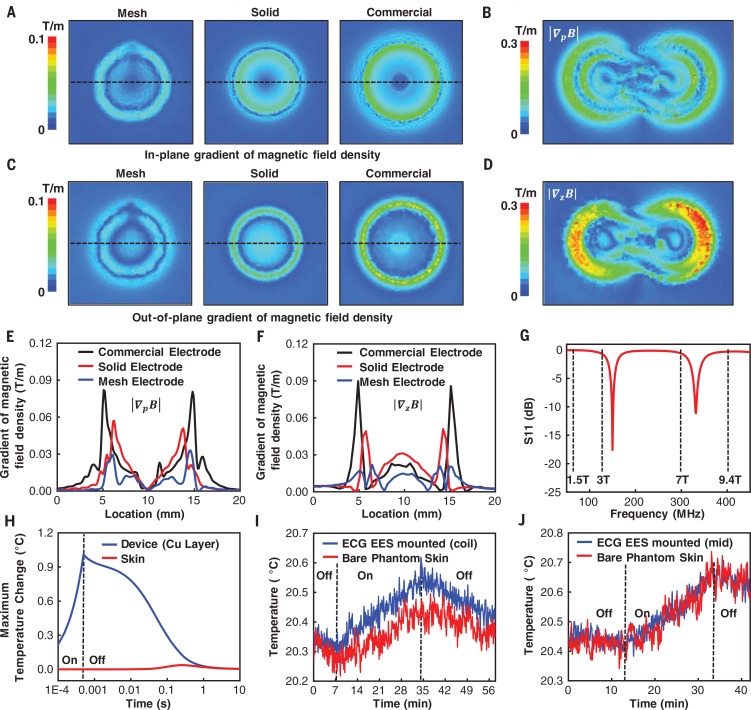
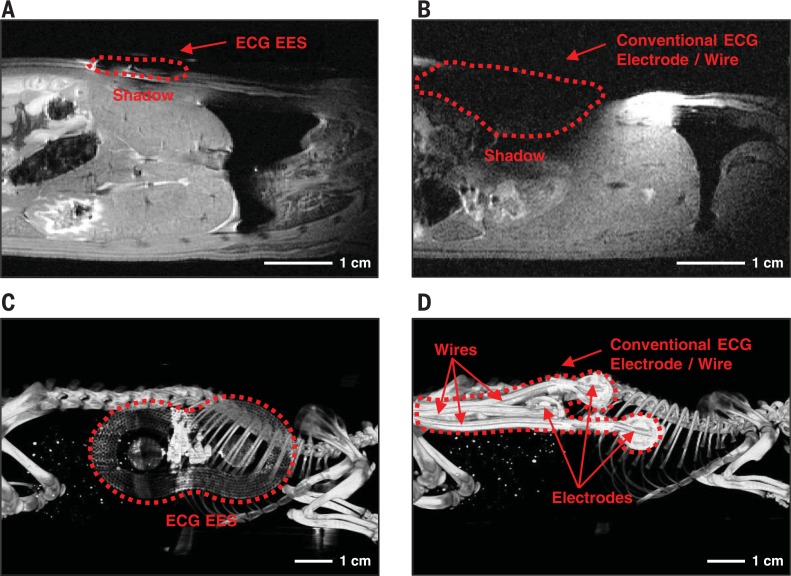
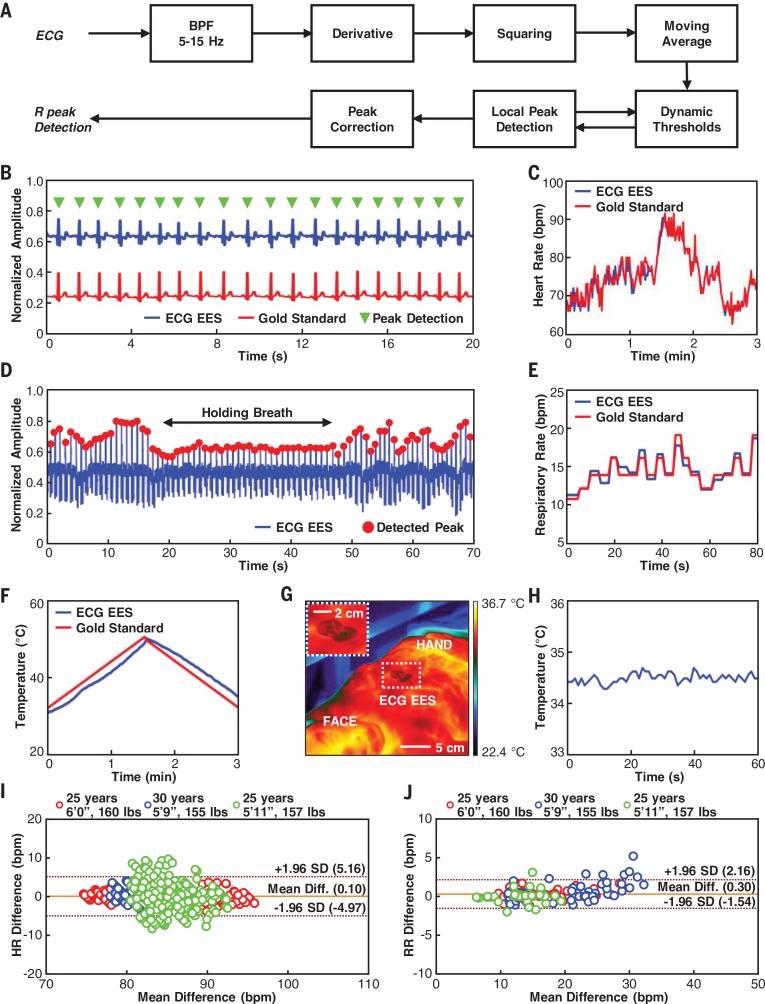
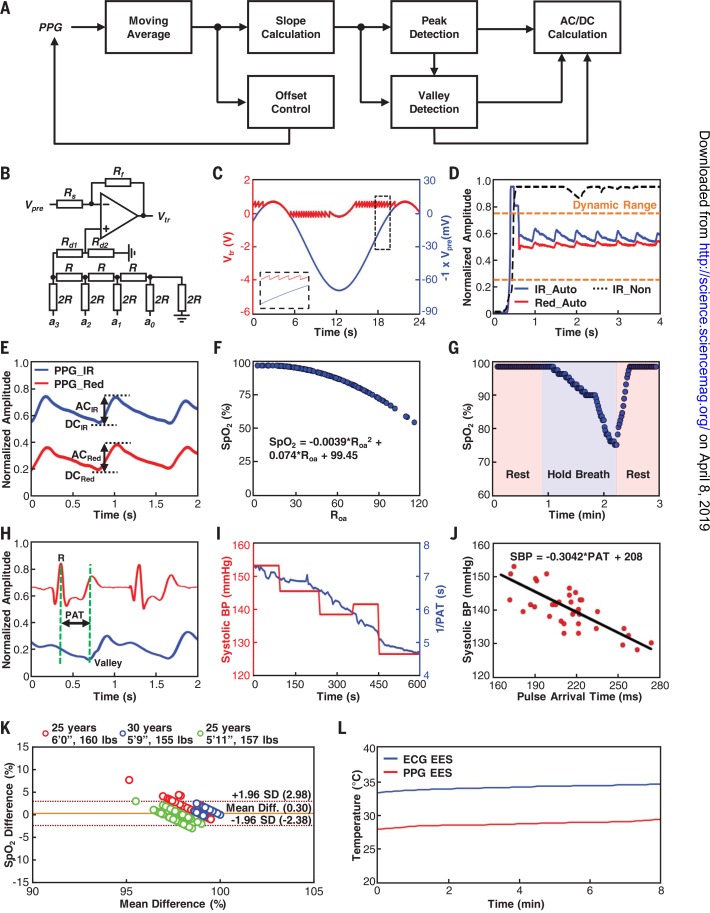
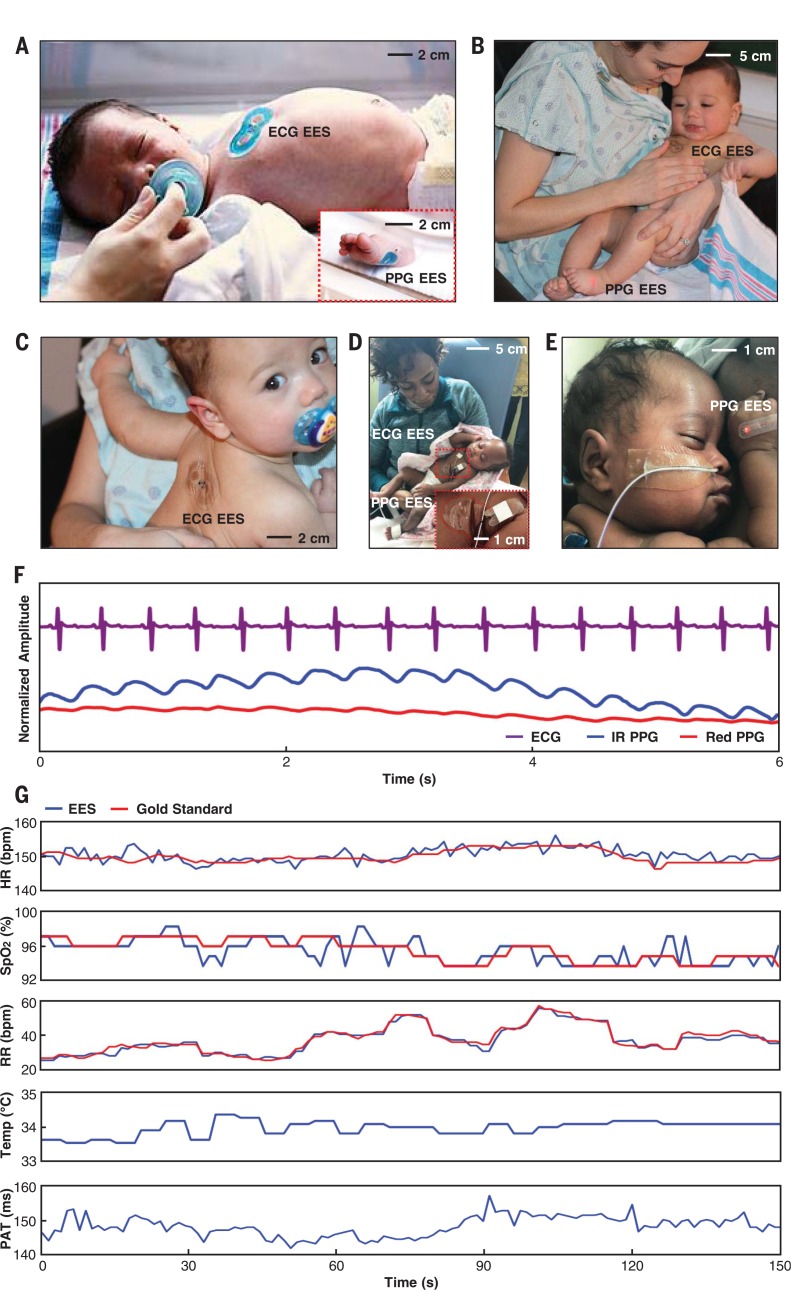
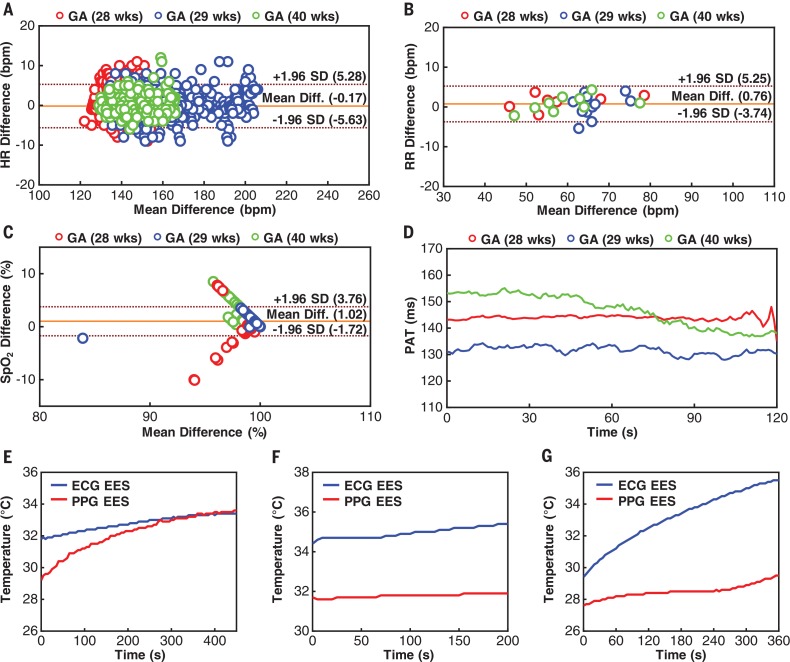
Existing vital sign monitoring systems in the neonatal intensive care unit (NICU) require multiple wires connected to rigid sensors with strongly adherent interfaces to the skin. We introduce a pair of ultrathin, soft, skin-like electronic devices whose coordinated, wireless operation reproduces the functionality of these traditional technologies but bypasses their intrinsic limitations. The enabling advances in engineering science include designs that support wireless, battery-free operation; real-time, in-sensor data analytics; time-synchronized, continuous data streaming; soft mechanics and gentle adhesive interfaces to the skin; and compatibility with visual inspection and with medical imaging techniques used in the NICU. Preliminary studies on neonates admitted to operating NICUs demonstrate performance comparable to the most advanced clinical-standard monitoring systems.
Copyright © 2019, American Association for the Advancement of Science.
Conflict of interest statement
H.U.C., B.H.K., J.Y.L., J.L., K.L., S.X., and J.A.R. are inventors on a patent application (U.S. 62/753,303) submitted by Northwestern University and the University of Illinois. H.U.C., S.X., and J.A.R. declare equity ownership in a company that is pursuing commercialization of the technology described here. J.A.R. also declares an advisory role with this company.
Figures
Comment in
-
Improving care of critically ill newborns.Science. 2019 Mar 1;363(6430):924-925. doi: 10.1126/science.aaw2085. Science. 2019. PMID: 30819947 No abstract available.
-
Wireless monitoring and artificial intelligence: A bright future in cardiothoracic surgery.J Thorac Cardiovasc Surg. 2020 Sep;160(3):809-812. doi: 10.1016/j.jtcvs.2019.08.141. Epub 2019 Dec 13. J Thorac Cardiovasc Surg. 2020. PMID: 31843227 No abstract available.
References
-
- Lund C., Medical adhesives in the NICU. Newborn Infant Nurs. Rev. 14, 160–165 (2014). doi: 10.1053/j.nainr.2014.10.001 - DOI
-
- Bouwstra S., Chen W., Feijs L., Oetomo S. B., in 2009 Sixth International Workshop on Wearable and Implantable Body Sensor Networks (IEEE, 2009), pp. 162–167. doi: 10.1109/BSN.2009.40 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
