

Evaluation of a surgical supervision model in three African countries-protocol for a prospective mixed-methods controlled pilot trial
- PMID: 30820336
- PMCID: PMC6378729
- DOI: 10.1186/s40814-019-0409-6
Evaluation of a surgical supervision model in three African countries-protocol for a prospective mixed-methods controlled pilot trial
Abstract
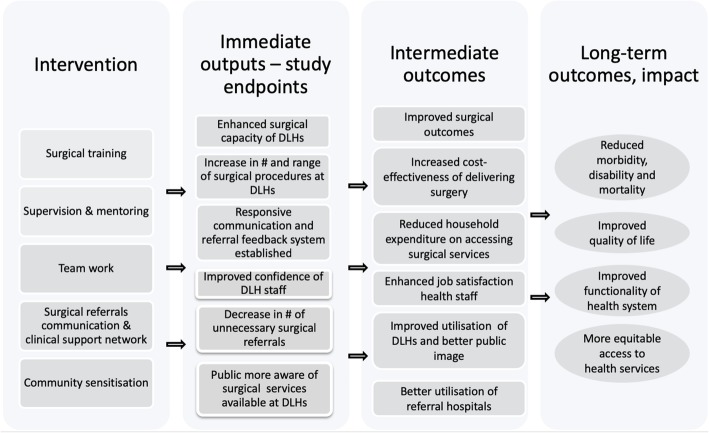
Background: District-level hospitals (DLHs) can play an important role in the delivery of essential surgical services for rural populations in sub-Saharan Africa if adequately prepared and supported. This article describes the protocol for the evaluation of the Scaling up Safe Surgery for District and Rural Populations in Africa (SURG-Africa) project which aims to strengthen the capacity in district-level hospitals (DLHs) in Malawi, Tanzania and Zambia to deliver safe, quality surgery. The intervention comprises a programme of quarterly supervisory visits to surgically active district-level hospitals by specialists from referral hospitals and the establishment of a mobile phone-based consultation network. The overall objective is to test and refine the model with a view to scaling up to national level.
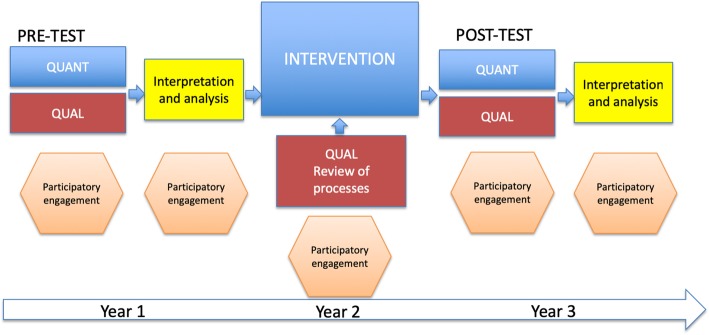
Methods: This mixed-methods controlled pilot trial will test the feasibility of the proposed supervision model in making quality-assured surgery available at DLHs. Firstly, the study will conduct a quantitative assessment of surgical service delivery at district facilities, looking at hospital preparedness, capacity and productivity, and how these are affected by the intervention. Secondly, the study will monitor changes in referral patterns from DLHs to a higher level of care as a result of the intervention. Data on utilisation of the mobile based-support network will also be collected. The analysis will compare changes over time and between intervention and control hospitals. The third element of the study will involve a qualitative assessment to obtain a better understanding of the functionality of DLH surgical systems and how these have been influenced by the intervention. It will also provide further information on feasibility, impact and sustainability of the supervision model.
Discussion: We seek to test a model of district-level capacity building through regular supervision by specialists and mobile phone technology-supported consultations to make safe surgical services more accessible, equitable and sustainable for rural populations in the target countries. The results of this study will provide robust evidence to inform and guide local actors in the national scale-up of the supervision model. Lessons learned will be transferred to the wider region.
Keywords: Africa; Evaluation; Non-physician clinicians; Supervision; Surgery; Surgical training.
Conflict of interest statement
Ethical approval for this study was granted by the Research Ethics Committee (REC) of the Royal College of Surgeons in Ireland, the project consortium lead, under approval no. REC 1417. In the implementation countries, ethical approval was received from the College of Medicine Research Ethics Committee in Malawi (approval no. P.05/17/2179), the University of Zambia Biomedical Research Ethics Committee (approval no. 005-05-17), the Kilimanjaro Christian Medical College Research Ethics and Review Committee (approval no. CRERC 2026) and the National Institute for Medical Research in Tanzania (approval no. NIMR/HQ/R.8a/Vol. IX/2600).Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Debas HT, Gosselin R, McCord C, et al. Surgery. In: Dean TJ, et al., editors. Disease control priorities in developing countries. 2. New York: The World Bank and Oxford University Press; 2006.
LinkOut - more resources
Full Text Sources
