

A simple high-throughput approach identifies actionable drug sensitivities in patient-derived tumor organoids
- PMID: 30820473
- PMCID: PMC6389967
- DOI: 10.1038/s42003-019-0305-x
A simple high-throughput approach identifies actionable drug sensitivities in patient-derived tumor organoids
Abstract
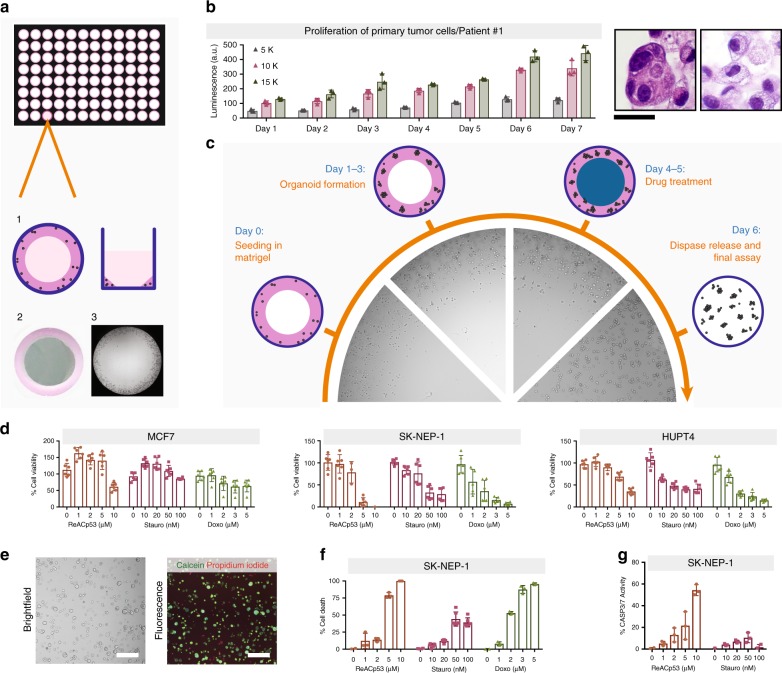
Tumor organoids maintain cell-cell interactions, heterogeneity, microenvironment, and drug response of the sample they originate from. Thus, there is increasing interest in developing tumor organoid models for drug development and personalized medicine applications. Although organoids are in principle amenable to high-throughput screenings, progress has been hampered by technical constraints and extensive manipulations required by current methods. Here we introduce a miniaturized method that uses a simplified geometry by seeding cells around the rim of the wells (mini-rings). This allows high-throughput screenings in a format compatible with automation as shown using four patient-derived tumor organoids established from two ovarian and one peritoneal high-grade serous carcinomas and one carcinosarcoma of the ovary. Using our automated screening platform, we identified personalized responses by measuring viability, number, and size of organoids after exposure to 240 kinase inhibitors. Results are available within a week from surgery, a timeline compatible with therapeutic decision-making.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Voest EE, Bernards R. DNA-guided precision medicine for cancer: a case of irrational exuberance? Cancer Discov. 2016;6:130–132. doi: 10.1158/2159-8290.CD-15-1321. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
