

CT-Based 3D Printing of the Glenoid Prior to Shoulder Arthroplasty: Bony Morphology and Model Evaluation
- PMID: 30820811
- PMCID: PMC6737174
- DOI: 10.1007/s10278-019-00177-4
CT-Based 3D Printing of the Glenoid Prior to Shoulder Arthroplasty: Bony Morphology and Model Evaluation
Abstract
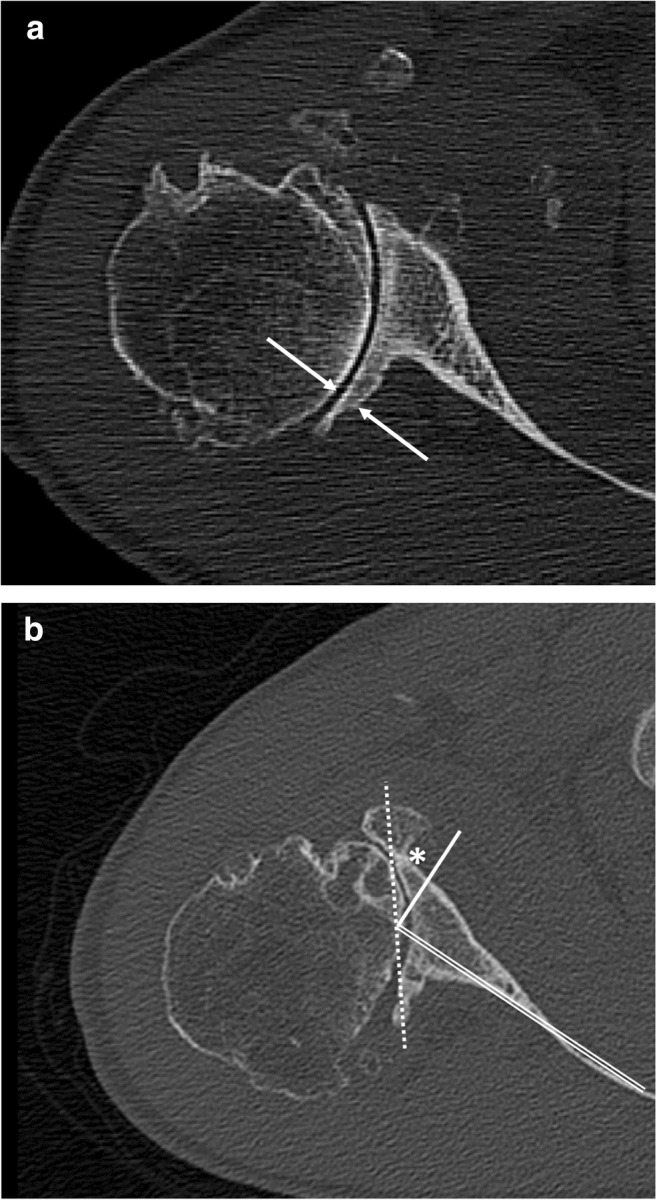
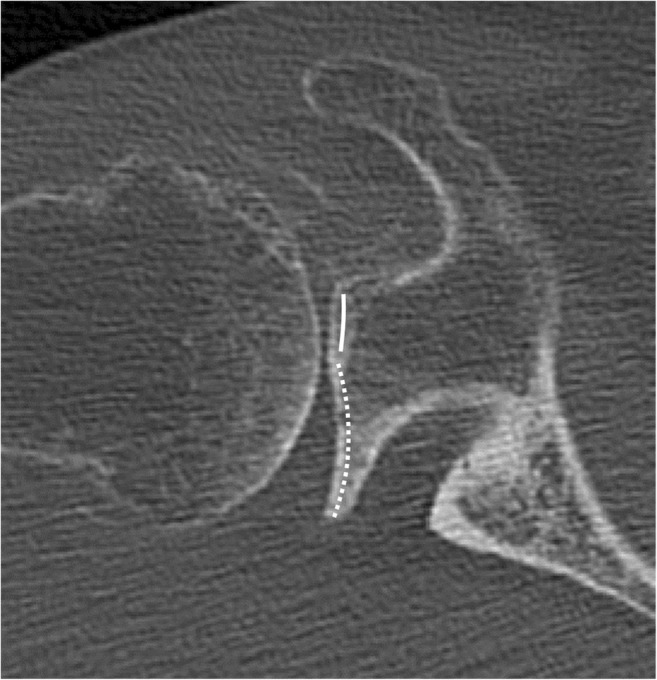
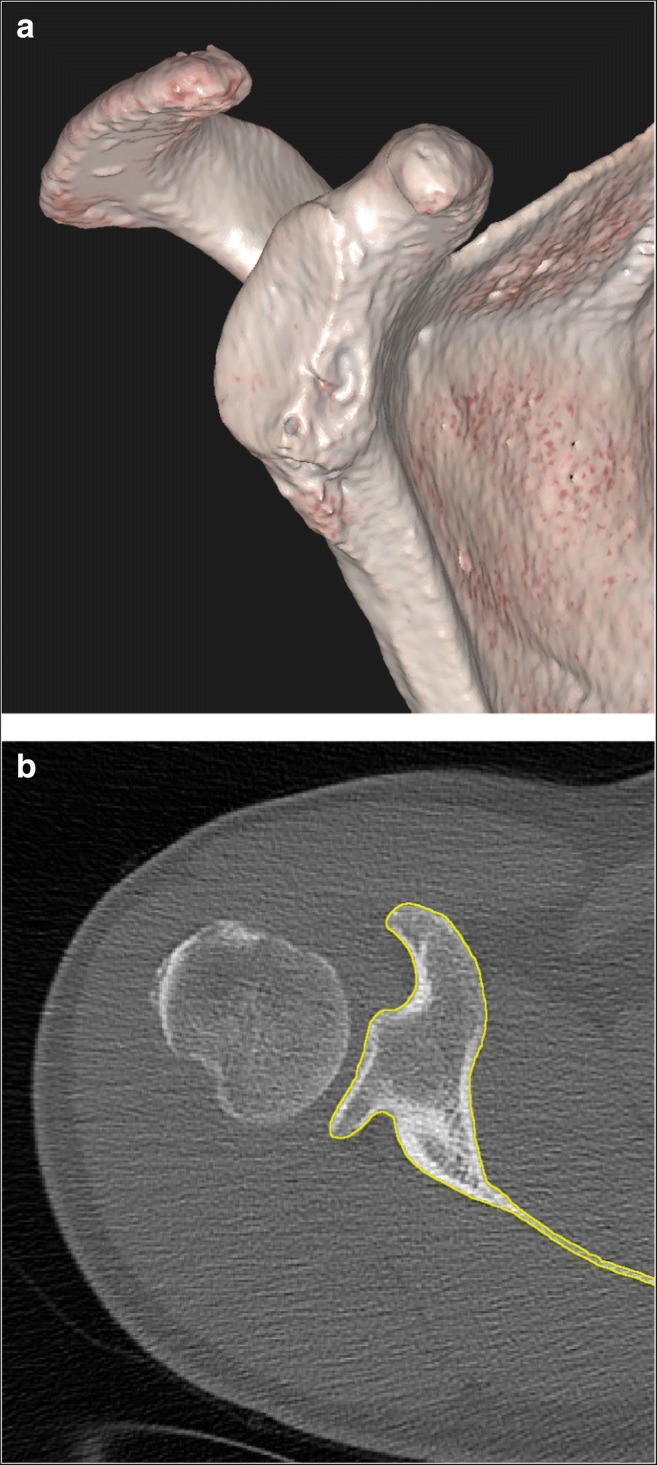
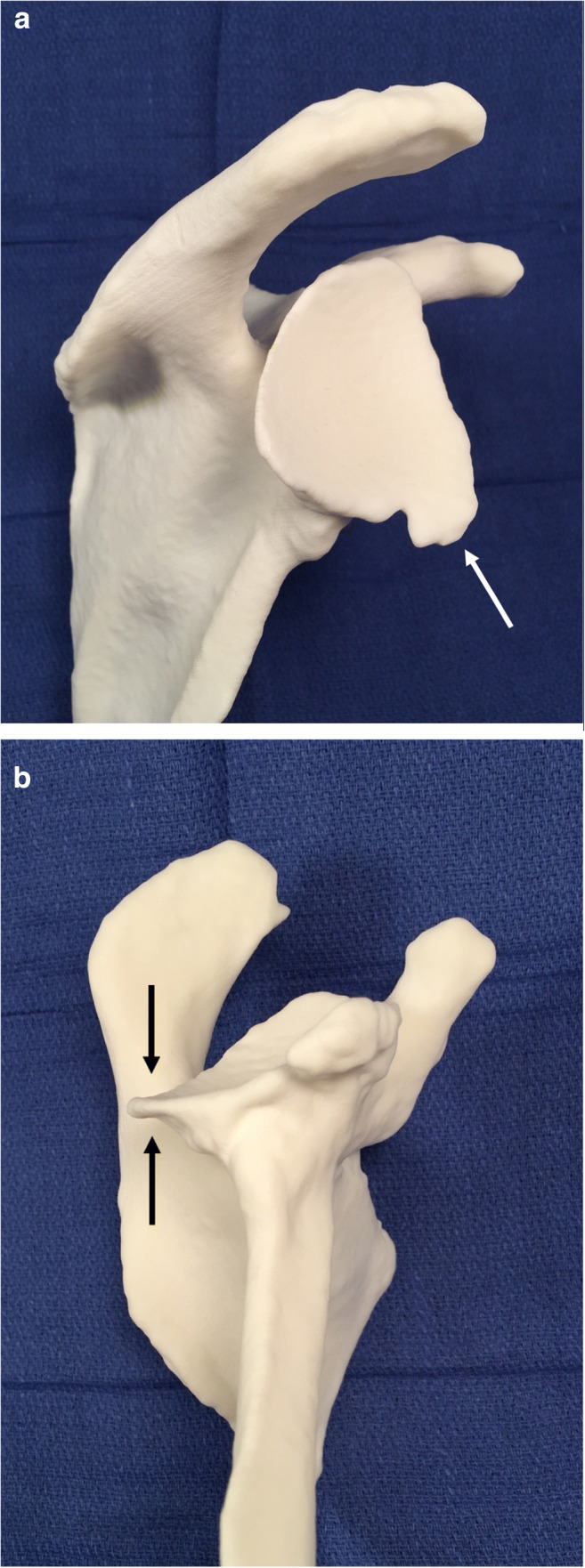
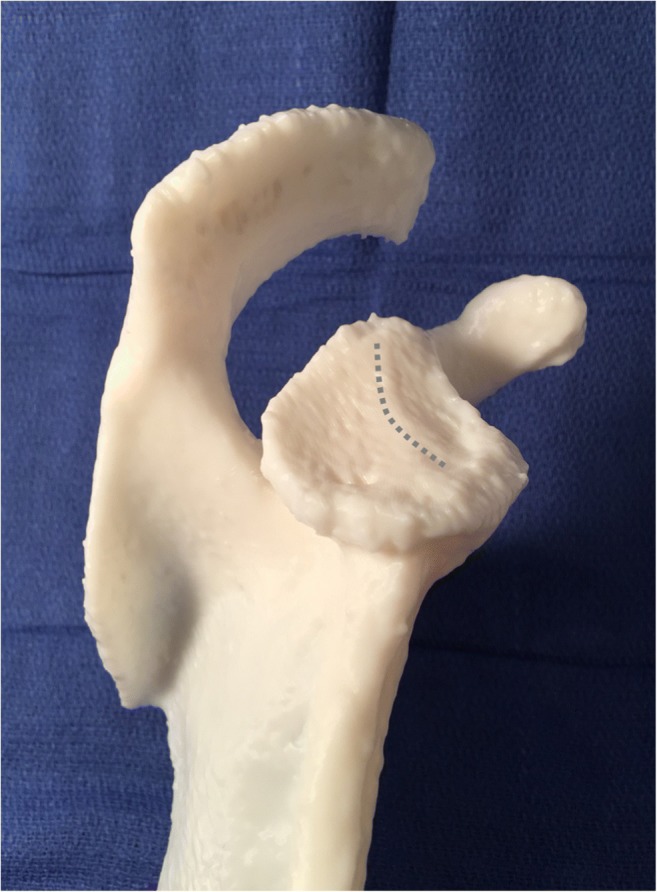
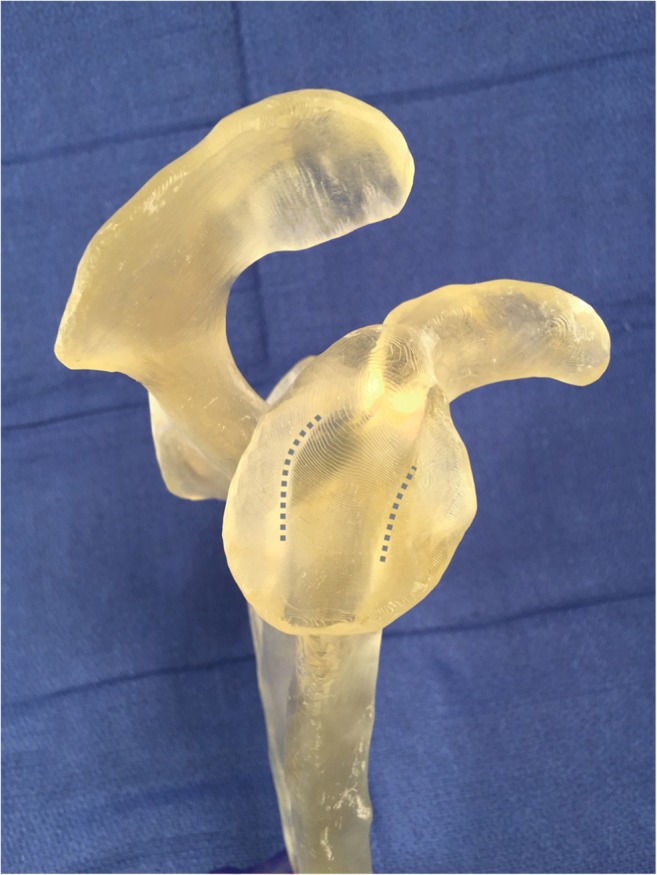
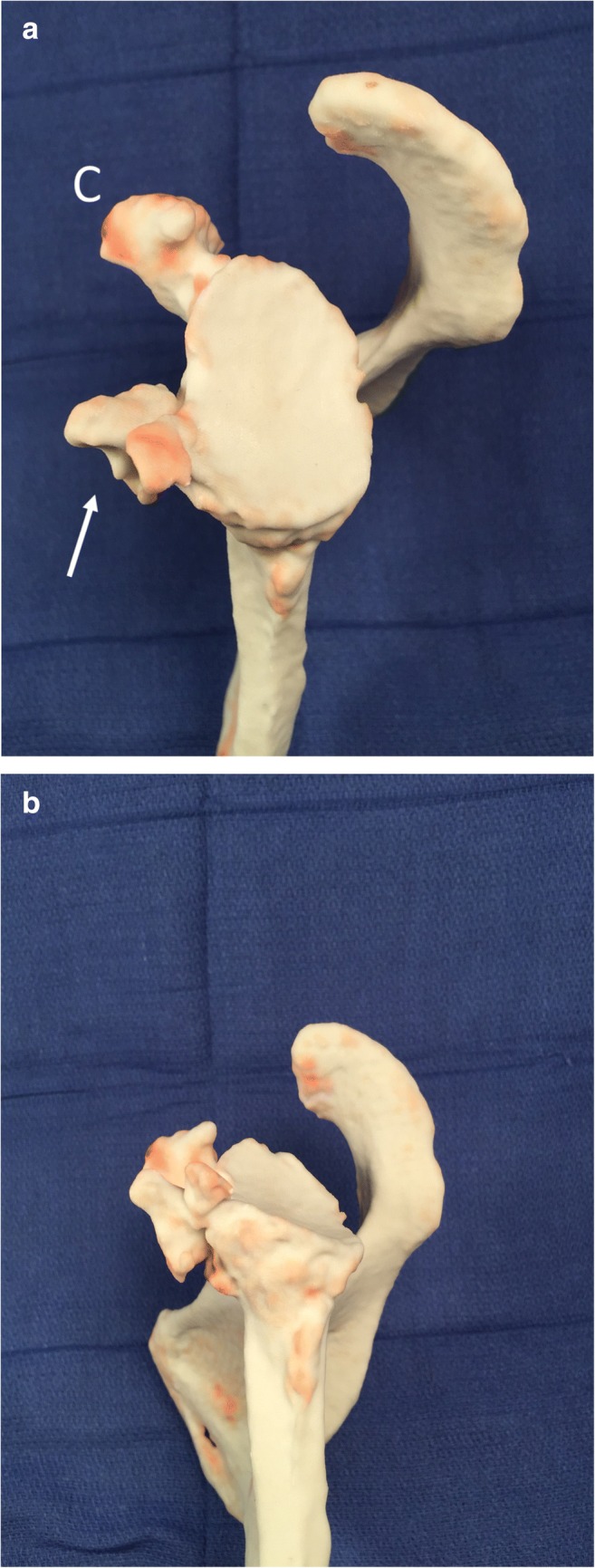
To demonstrate the 3D printed appearance of glenoid morphologies relevant to shoulder replacement surgery and to evaluate the benefits of printed models of the glenoid with regard to surgical planning. A retrospective review of patients referred for shoulder CT was performed, leading to a cohort of nine patients without arthroplasty hardware and exhibiting glenoid changes relevant to shoulder arthroplasty planning. Thin slice CT images were used to create both humerus-subtracted volume renderings of the glenoid, as well as 3D surface models of the glenoid, and 11 printed models were created. Volume renderings, surface models, and printed models were reviewed by a musculoskeletal radiologist for accuracy. Four fellowship-trained orthopaedic surgeons specializing in shoulder surgery reviewed each case individually as follows: First, the source CT images were reviewed, and a score for the clarity of the bony morphologies relevant to shoulder arthroplasty surgery was given. The volume rendering was reviewed, and the clarity was again scored. Finally, the printed model was reviewed, and the clarity again scored. Each printed model was also scored for morphologic complexity, expected usefulness of the printed model, and physical properties of the model. Mann-Whitney-Wilcoxon signed rank tests of the clarity scores were calculated, and the Spearman's ρ correlation coefficient between complexity and usefulness scores was computed. Printed models demonstrated a range of glenoid bony changes including osteophytes, glenoid bone loss, retroversion, and biconcavity. Surgeons rated the glenoid morphology as more clear after review of humerus-subtracted volume rendering, compared with review of the source CT images (p = 0.00903). Clarity was also better with 3D printed models compared to CT (p = 0.00903) and better with 3D printed models compared to humerus-subtracted volume rendering (p = 0. 00879). The expected usefulness of printed models demonstrated a positive correlation with morphologic complexity, with Spearman's ρ 0.73 (p = 0.0108). 3D printing of the glenoid based on pre-operative CT provides a physical representation of patient anatomy. Printed models enabled shoulder surgeons to appreciate glenoid bony morphology more clearly compared to review of CT images or humerus-subtracted volume renderings. These models were more useful as glenoid complexity increased.
Keywords: 3D printing; Computed tomography; Glenoid morphology; Shoulder arthroplasty; Surgical planning.
Conflict of interest statement
3D Systems provided access to the DICOM-to-Print software and also printed one model presented in this work. The authors retained full control of all aspects of the study. One author reports grant funding from the Department of Veterans Affairs, and the Orthopaedic Research and Education Foundation, for other work relating to shoulder disorders. Another author reports grant funding from the National Center for Defense Manufacturing and Machining for other work relating to 3D printing.
Figures

Similar articles
-
Glenoid bony morphology of osteoarthritis prior to shoulder arthroplasty: what the surgeon wants to know and why.Skeletal Radiol. 2021 May;50(5):881-894. doi: 10.1007/s00256-020-03647-x. Epub 2020 Oct 23. Skeletal Radiol. 2021. PMID: 33095290 Review.
-
Clinical and radiologic outcomes of Lima ProMade custom 3D-printed glenoid components in primary and revision reverse total shoulder arthroplasty with severe glenoid bone loss: a minimum 2-year follow-up.J Shoulder Elbow Surg. 2023 Oct;32(10):2017-2026. doi: 10.1016/j.jse.2023.04.020. Epub 2023 May 30. J Shoulder Elbow Surg. 2023. PMID: 37263477
-
The influence of three-dimensional planning on decision-making in total shoulder arthroplasty.J Shoulder Elbow Surg. 2017 Aug;26(8):1477-1483. doi: 10.1016/j.jse.2017.01.006. Epub 2017 Feb 2. J Shoulder Elbow Surg. 2017. PMID: 28162884
-
3-dimensionally printed patient-specific glenoid drill guides vs. standard nonspecific instrumentation: a randomized controlled trial comparing the accuracy of glenoid component placement in anatomic total shoulder arthroplasty.J Shoulder Elbow Surg. 2024 Feb;33(2):223-233. doi: 10.1016/j.jse.2023.08.014. Epub 2023 Sep 27. J Shoulder Elbow Surg. 2024. PMID: 37774830 Clinical Trial.
-
Inconsistencies in measuring glenoid version in shoulder arthroplasty: a systematic review.J Shoulder Elbow Surg. 2025 Feb;34(2):639-649. doi: 10.1016/j.jse.2024.08.020. Epub 2024 Oct 9. J Shoulder Elbow Surg. 2025. PMID: 39389450
Cited by
-
Advanced 3D Visualization and 3D Printing in Radiology.Adv Exp Med Biol. 2023;1406:103-138. doi: 10.1007/978-3-031-26462-7_6. Adv Exp Med Biol. 2023. PMID: 37016113
-
Shoulder Reconstruction Using a 3D Printed 'Gigaprosthesis' Following Resection of Massive Primary Bone Tumour.Indian J Surg Oncol. 2024 Dec;15(4):738-745. doi: 10.1007/s13193-024-02042-5. Epub 2024 Jul 30. Indian J Surg Oncol. 2024. PMID: 39555371 No abstract available.
-
Comparison of Glenoid Dimensions Between 3D Computed Tomography and 3D Printing.Cureus. 2024 Jan 28;16(1):e53133. doi: 10.7759/cureus.53133. eCollection 2024 Jan. Cureus. 2024. PMID: 38420064 Free PMC article.
-
Restoring Rotation Center in Total Hip Arthroplasty for Developmental Dysplasia of the Hip with the Assistance of Three Dimensional Printing Technology: A Pilot Study.Orthop Surg. 2022 Jan;14(1):119-128. doi: 10.1111/os.13183. Epub 2021 Dec 13. Orthop Surg. 2022. PMID: 34898037 Free PMC article.
-
Glenoid bony morphology of osteoarthritis prior to shoulder arthroplasty: what the surgeon wants to know and why.Skeletal Radiol. 2021 May;50(5):881-894. doi: 10.1007/s00256-020-03647-x. Epub 2020 Oct 23. Skeletal Radiol. 2021. PMID: 33095290 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
