

Experience of extracorporeal cardiopulmonary resuscitation in a refractory cardiac arrest patient at the emergency department
- PMID: 30820972
- PMCID: PMC6712328
- DOI: 10.1002/clc.23169
Experience of extracorporeal cardiopulmonary resuscitation in a refractory cardiac arrest patient at the emergency department
Abstract
Background: Extracorporeal cardiopulmonary resuscitation (ECPR) is a method to improve survival outcomes in refractory cardiac arrest.
Hypothesis: This study aimed to determine the associated factors related to outcome and to analyze the post-ECPR management in patients who received ECPR due to nonresponse to advanced cardiac life support (ACLS).
Methods: This was a retrospective analysis based on a prospective cohort. Cardiac arrest patients who received ECPR in our emergency department from May 2006 to December 2017 were selected from the prospective cohort. Patients who received ECPR for rearrest were excluded. The primary outcome was survival to discharge.
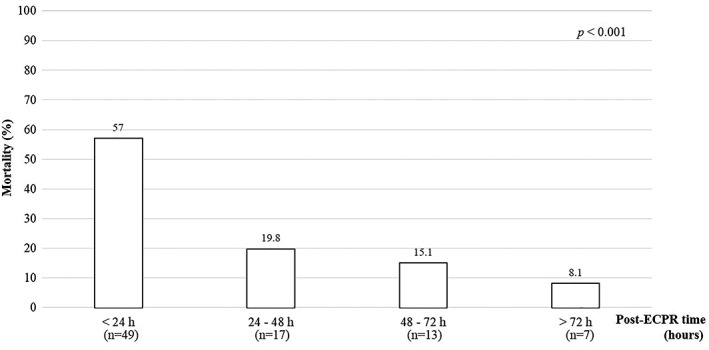
Results: ECPR was attempted in 100 patients who did not respond to ACLS. Fourteen patients survived to discharge, and 12 (85.7%) patients showed good neurologic outcomes. The rate of survival to discharge decreased according to increasing age and ACLS duration. Age, presence of any return of spontaneous circulation (ROSC) during ACLS, and prolongation of ACLS were associated factors for survival discharge in ECPR patients. Fourteen patients required distal perfusion catheters, and 35 patients received continuous renal replacement therapy (CRRT). The proportion of death was the highest within 24 hours after ECPR as 57.0%.
Conclusions: The early transition from ACLS to ECPR may improve the ECPR outcomes. In addition, good outcomes are expected for ECPR performed after refractory arrest if the patient is young and experiences an ROSC event during ACLS. In post ECPR management, the majority of mortality events were occurred in the early period, and distal perfusion catheter and CRRT were frequently required.
Keywords: advanced cardiac life support; emergency department; extracorporeal cardiopulmonary resuscitation; refractory cardiac arrest.
© 2019 The Authors. Clinical Cardiology published by Wiley Periodicals, Inc.
Conflict of interest statement
Authors' contributions
K.S.H., S.J.K., and S.W.L. conceived the study design and wrote the manuscript. E.J.L., J.S.J., J.H.P., J.S.P., and K.S.H. were responsible for patient care and helped conduct the trial and data collection. K.S.H. and S.W.L. managed and analyzed the data, including quality control. All authors contributed substantially to the revision of the manuscript.
Figures


Similar articles
-
Extracorporeal versus conventional cardiopulmonary resuscitation for refractory out-of-hospital cardiac arrest: a secondary analysis of the Prague OHCA trial.Crit Care. 2022 Oct 27;26(1):330. doi: 10.1186/s13054-022-04199-3. Crit Care. 2022. PMID: 36303227 Free PMC article. Clinical Trial.
-
Managing cardiac arrest with refractory ventricular fibrillation in the emergency department: Conventional cardiopulmonary resuscitation versus extracorporeal cardiopulmonary resuscitation.Resuscitation. 2015 Jul;92:70-6. doi: 10.1016/j.resuscitation.2015.04.016. Epub 2015 Apr 29. Resuscitation. 2015. PMID: 25936930
-
Neurological outcomes and duration from cardiac arrest to the initiation of extracorporeal membrane oxygenation in patients with out-of-hospital cardiac arrest: a retrospective study.Scand J Trauma Resusc Emerg Med. 2017 Sep 16;25(1):95. doi: 10.1186/s13049-017-0440-7. Scand J Trauma Resusc Emerg Med. 2017. PMID: 28915913 Free PMC article.
-
Comparing extracorporeal cardiopulmonary resuscitation with conventional cardiopulmonary resuscitation: A meta-analysis.Resuscitation. 2016 Jun;103:106-116. doi: 10.1016/j.resuscitation.2016.01.019. Epub 2016 Feb 2. Resuscitation. 2016. PMID: 26851058 Review.
-
Extracorporeal membrane oxygenation for refractory cardiac arrest.Ann Card Anaesth. 2017 Jan;20(Supplement):S4-S10. doi: 10.4103/0971-9784.197790. Ann Card Anaesth. 2017. PMID: 28074817 Free PMC article. Review.
Cited by
-
Controlled automated reperfusion of the whole body after cardiac arrest.J Thorac Dis. 2019 Jun;11(Suppl 10):S1464-S1470. doi: 10.21037/jtd.2019.04.05. J Thorac Dis. 2019. PMID: 31293795 Free PMC article.
-
Predictors of Survival and Favorable Neurologic Outcome in Patients Treated with eCPR: a Systematic Review and Meta-analysis.J Cardiovasc Transl Res. 2022 Apr;15(2):279-290. doi: 10.1007/s12265-021-10195-9. Epub 2022 Feb 22. J Cardiovasc Transl Res. 2022. PMID: 35194733
-
eCPR Combined With Therapeutic Hypothermia Could Improve Survival and Neurologic Outcomes for Patients With Cardiac Arrest: A Meta-Analysis.Front Cardiovasc Med. 2021 Aug 13;8:703567. doi: 10.3389/fcvm.2021.703567. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34485403 Free PMC article.
-
Complete percutaneous angio-guided approach using preclosing for venoarterial extracorporeal membrane oxygenation implantation and explantation in patients with refractory cardiogenic shock or cardiac arrest.Crit Care. 2021 Mar 7;25(1):93. doi: 10.1186/s13054-021-03522-8. Crit Care. 2021. PMID: 33678169 Free PMC article.
-
Extracorporeal cardiopulmonary resuscitation for adults with shock-refractory cardiac arrest.J Am Coll Emerg Physicians Open. 2021 Jan 18;2(1):e12361. doi: 10.1002/emp2.12361. eCollection 2021 Feb. J Am Coll Emerg Physicians Open. 2021. PMID: 33506232 Free PMC article. Review.
References
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in‐hospital cardiac arrest among children and adults. JAMA. 2006;295(1):50‐57. - PubMed
-
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of cardiopulmonary resuscitation. Resuscitation. 2003;58(3):297‐308. - PubMed
-
- Guidelines for indications for the use of extracorporeal life support in refractory cardiac arrest. French Ministry of Health. Ann Fr Anesth Reanim. 2009;28(2):182‐190. - PubMed
-
- Lim CH, Son HS, Baek KJ, et al. Comparison of coronary artery blood flow and hemodynamic energy in a pulsatile pump versus a combined nonpulsatile pump and an intra‐aortic balloon pump. ASAIO J. 2006;52(5):595‐597. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
