

Medical Doctors' Offline Computer-Assisted Digital Education: Systematic Review by the Digital Health Education Collaboration
- PMID: 30821689
- PMCID: PMC6418481
- DOI: 10.2196/12998
Medical Doctors' Offline Computer-Assisted Digital Education: Systematic Review by the Digital Health Education Collaboration
Abstract
Background: The widening gap between innovations in the medical field and the dissemination of such information to doctors may affect the quality of care. Offline computer-based digital education (OCDE) may be a potential solution to overcoming the geographical, financial, and temporal obstacles faced by doctors.
Objective: The objectives of this systematic review were to evaluate the effectiveness of OCDE compared with face-to-face learning, no intervention, or other types of digital learning for improving medical doctors' knowledge, cognitive skills, and patient-related outcomes. Secondary objectives were to assess the cost-effectiveness (CE) of OCDE and any adverse effects.
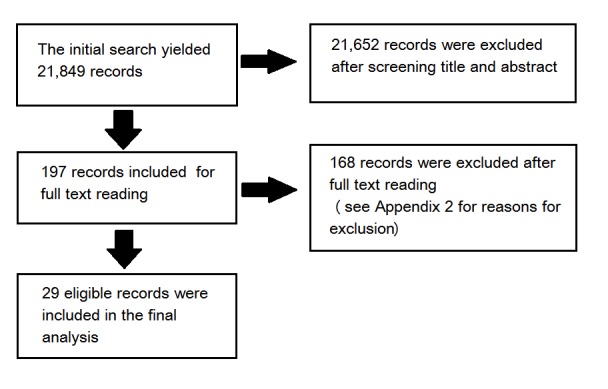
Methods: We searched major bibliographic databases from 1990 to August 2017 to identify relevant articles and followed the Cochrane methodology for systematic reviews of intervention.
Results: Overall, 27 randomized controlled trials (RCTs), 1 cluster RCT (cRCT), and 1 quasi-RCT were included in this review. The total number of participants was 1690 in addition to the cRCT, which included 24 practices. Due to the heterogeneity of the participants, interventions, and outcomes, meta-analysis was not feasible, and the results were presented as narrative summary. Compared with face-to-face learning, the effect of OCDE on knowledge gain is uncertain (ratio of the means [RM] range 0.95-1.17; 8 studies, 495 participants; very low grade of evidence). From the same comparison, the effect of OCDE on cognitive skill gain is uncertain (RM range 0.1-0.9; 8 studies, 375 participants; very low grade of evidence). OCDE may have little or no effect on patients' outcome compared with face-to-face education (2 studies, 62 participants; low grade of evidence). Compared with no intervention, OCDE may improve knowledge gain (RM range 1.36-0.98; 4 studies, 401 participants; low grade of evidence). From the same comparison, the effect of OCDE on cognitive skill gain is uncertain (RM range 1.1-1.15; 4 trials, 495 participants; very low grade of evidence). One cRCT, involving 24 practices, investigated patients' outcome in this comparison and showed no difference between the 2 groups with low-grade evidence. Compared with text-based learning, the effect of OCDE on cognitive skills gain is uncertain (RM range 0.91-1.46; 3 trials with 4 interventions; 68 participants; very low-grade evidence). No study in this comparison investigated knowledge gain or patients' outcomes. One study assessed the CE and showed that OCDE was cost-effective when compared with face-to-face learning if the cost is less than or equal to Can $200. No trial evaluated the adverse effect of OCDE.
Conclusions: The effect of OCDE compared with other methods of education on medical doctors' knowledge and cognitive skill gain is uncertain. OCDE may improve doctors' knowledge compared with no intervention but its effect on doctors' cognitive skills is uncertain. OCDE may have little or no effect in improving patients' outcome.
Keywords: medical education, digital education; systematic review.
©Hayfaa Abdelmageed Wahabi, Samia Ahmed Esmaeil, Khawater Hassan Bahkali, Maher Abdelraheim Titi, Yasser Sami Amer, Amel Ahmed Fayed, Amr Jamal, Nasriah Zakaria, Amna Rehana Siddiqui, Monika Semwal, Lorainne Tudor Car, Paul Posadzki, Josip Car. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 01.03.2019.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Offline Digital Education for Postregistration Health Professions: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration.J Med Internet Res. 2019 Apr 24;21(4):e12968. doi: 10.2196/12968. J Med Internet Res. 2019. PMID: 31017584 Free PMC article.
-
Online Digital Education for Postregistration Training of Medical Doctors: Systematic Review by the Digital Health Education Collaboration.J Med Internet Res. 2019 Feb 25;21(2):e13269. doi: 10.2196/13269. J Med Internet Res. 2019. PMID: 30801252 Free PMC article.
-
Digital Health Professions Education in the Field of Pediatrics: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration.J Med Internet Res. 2019 Sep 25;21(9):e14231. doi: 10.2196/14231. J Med Internet Res. 2019. PMID: 31573906 Free PMC article.
-
Effectiveness of Digital Education on Communication Skills Among Medical Students: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration.J Med Internet Res. 2019 Aug 27;21(8):e12967. doi: 10.2196/12967. J Med Internet Res. 2019. PMID: 31456579 Free PMC article.
-
Offline Digital Education for Medical Students: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration.J Med Internet Res. 2019 Mar 25;21(3):e13165. doi: 10.2196/13165. J Med Internet Res. 2019. PMID: 30907731 Free PMC article.
Cited by
-
Digital Education for the Management of Chronic Wounds in Health Care Professionals: Protocol for a Systematic Review by the Digital Health Education Collaboration.JMIR Res Protoc. 2019 Mar 25;8(3):e12488. doi: 10.2196/12488. JMIR Res Protoc. 2019. PMID: 30907743 Free PMC article.
-
Use of digital technologies for staff education and training programmes on newborn resuscitation and complication management: a scoping review.BMJ Paediatr Open. 2024 May 15;8(1):e002105. doi: 10.1136/bmjpo-2023-002105. BMJ Paediatr Open. 2024. PMID: 38754893 Free PMC article.
-
Digital Education for Health Professionals: An Evidence Map, Conceptual Framework, and Research Agenda.J Med Internet Res. 2022 Mar 17;24(3):e31977. doi: 10.2196/31977. J Med Internet Res. 2022. PMID: 35297767 Free PMC article. Review.
-
Spaced Digital Education for Health Professionals: Systematic Review and Meta-Analysis.J Med Internet Res. 2024 Oct 10;26:e57760. doi: 10.2196/57760. J Med Internet Res. 2024. PMID: 39388234 Free PMC article.
-
Offline Digital Education for Postregistration Health Professions: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration.J Med Internet Res. 2019 Apr 24;21(4):e12968. doi: 10.2196/12968. J Med Internet Res. 2019. PMID: 31017584 Free PMC article.
References
-
- Lawton S, Wimpenny P. Continuing professional development: a review. Nurs Stand. 2003;17(24):41–4. - PubMed
-
- O'Neil KM, Addrizzo-Harris DJ, American College of Chest Physicians Health and Science Policy Committee Continuing medical education effect on physician knowledge application and psychomotor skills: effectiveness of continuing medical education: American College of Chest Physicians Evidence–Based Educational Guidelines. Chest. 2009 Mar;135(3 Suppl):37S–41S. doi: 10.1378/chest.08-2516.S0012-3692(09)60172-0 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
