Effectiveness of Implementing a Collaborative Chronic Care Model for Clinician Teams on Patient Outcomes and Health Status in Mental Health: A Randomized Clinical Trial
- PMID: 30821830
- PMCID: PMC6484628
- DOI: 10.1001/jamanetworkopen.2019.0230
Effectiveness of Implementing a Collaborative Chronic Care Model for Clinician Teams on Patient Outcomes and Health Status in Mental Health: A Randomized Clinical Trial
Abstract
Importance: Collaborative chronic care models (CCMs) have extensive randomized clinical trial evidence for effectiveness in serious mental illnesses, but little evidence exists regarding their feasibility or effect in typical practice conditions.
Objective: To determine the effectiveness of implementation facilitation in establishing the CCM in mental health teams and the impact on health outcomes of team-treated individuals.
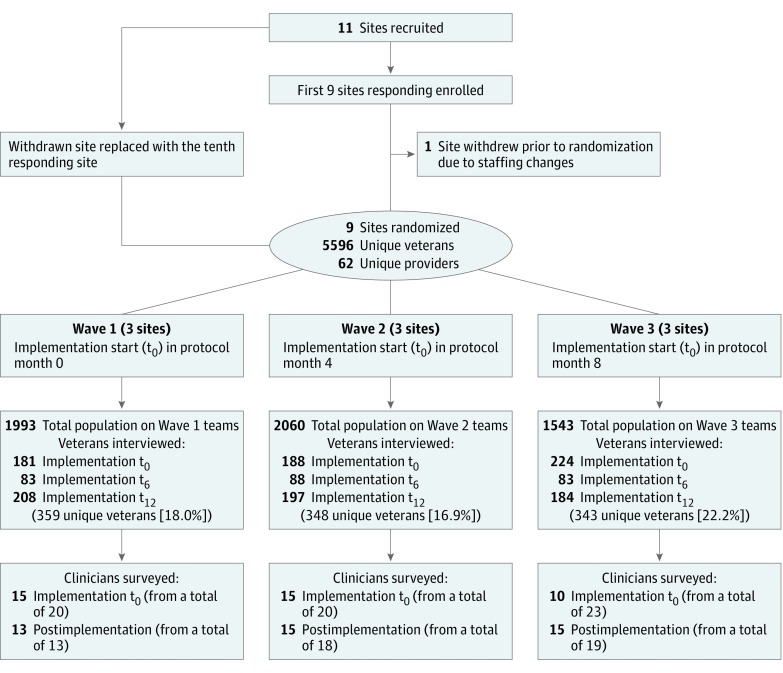
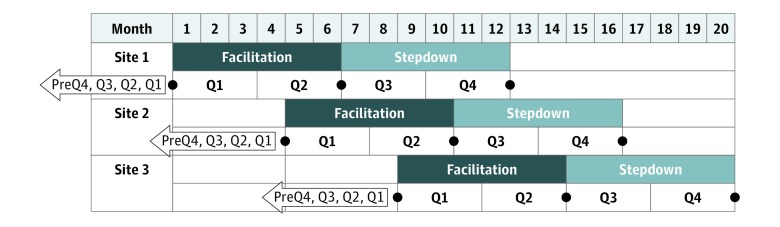
Design, setting, and participants: This quasi-experimental, randomized stepped-wedge implementation trial was conducted from February 2016 through February 2018, in partnership with the US Department of Veterans Affairs (VA) Office of Mental Health and Suicide Prevention. Nine facilities were enrolled from all VA facilities in the United States to receive CCM implementation support. All veterans (n = 5596) treated by designated outpatient general mental health teams were included for hospitalization analyses, and a randomly selected sample (n = 1050) was identified for health status interviews. Individuals with dementia were excluded. Clinicians (n = 62) at the facilities were surveyed, and site process summaries were rated for concordance with the CCM process. The CCM implementation start time was randomly assigned across 3 waves. Data analysis of this evaluable population was performed from June to September 2018.
Interventions: Internal-external facilitation, combining a study-funded external facilitator and a facility-funded internal facilitator working with a designated team for 1 year.
Main outcomes and measures: Facilitation was hypothesized to be associated with improvements in both implementation and intervention outcomes (hybrid type II trial). Implementation outcomes included the clinician Team Development Measure (TDM) and proportion of CCM-concordant team care processes. The study was powered for the primary health outcome, mental component score (MCS). Hospitalization rate was derived from administrative data.
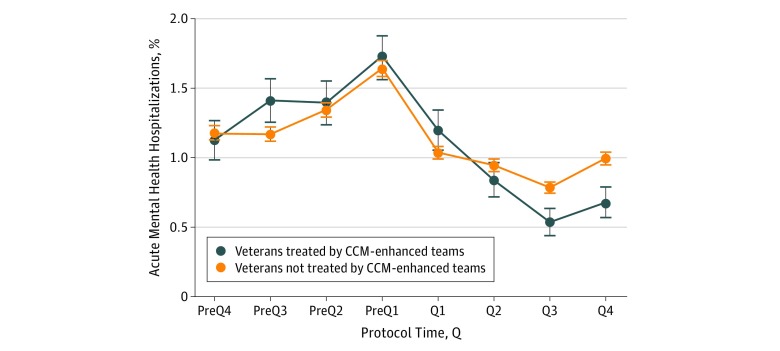
Results: The veteran population (n = 5596) included 881 women (15.7%), and the mean (SD) age was 52.2 (14.5) years. The interviewed sample (n = 1050) was similar but was oversampled for women (n = 210 [20.0%]). Facilitation was associated with improvements in TDM subscales for role clarity (53.4%-68.6%; δ = 15.3; 95% CI, 4.4-26.2; P = .01) and team primacy (50.0%-68.6%; δ = 18.6; 95% CI, 8.3-28.9; P = .001). The percentage of CCM-concordant processes achieved varied, ranging from 44% to 89%. No improvement was seen in veteran self-ratings, including the primary outcome. In post hoc analyses, MCS improved in veterans with 3 or more treated mental health diagnoses compared with others (β = 5.03; 95% CI, 2.24-7.82; P < .001). Mental health hospitalizations demonstrated a robust decrease during facilitation (β = -0.12; 95% CI, -0.16 to -0.07; P < .001); this finding withstood 4 internal validity tests.
Conclusions and relevance: Implementation facilitation that engages clinicians under typical practice conditions can enhance evidence-based team processes; its effect on self-reported overall population health status was negligible, although health status improved for individuals with complex conditions and hospitalization rate declined.
Trial registration: ClinicalTrials.gov Identifier: NCT02543840.
Conflict of interest statement
Figures