

Comparative study of simulated nebulized and spray particle deposition in chronic rhinosinusitis patients
- PMID: 30821929
- PMCID: PMC7457377
- DOI: 10.1002/alr.22324
Comparative study of simulated nebulized and spray particle deposition in chronic rhinosinusitis patients
Abstract
Background: Topical intranasal drugs are widely prescribed for chronic rhinosinusitis (CRS), although delivery can vary with device type and droplet size. The study objective was to compare nebulized and sprayed droplet deposition in the paranasal sinuses and ostiomeatal complex (OMC) across multiple droplet sizes in CRS patients using computational fluid dynamics (CFD).
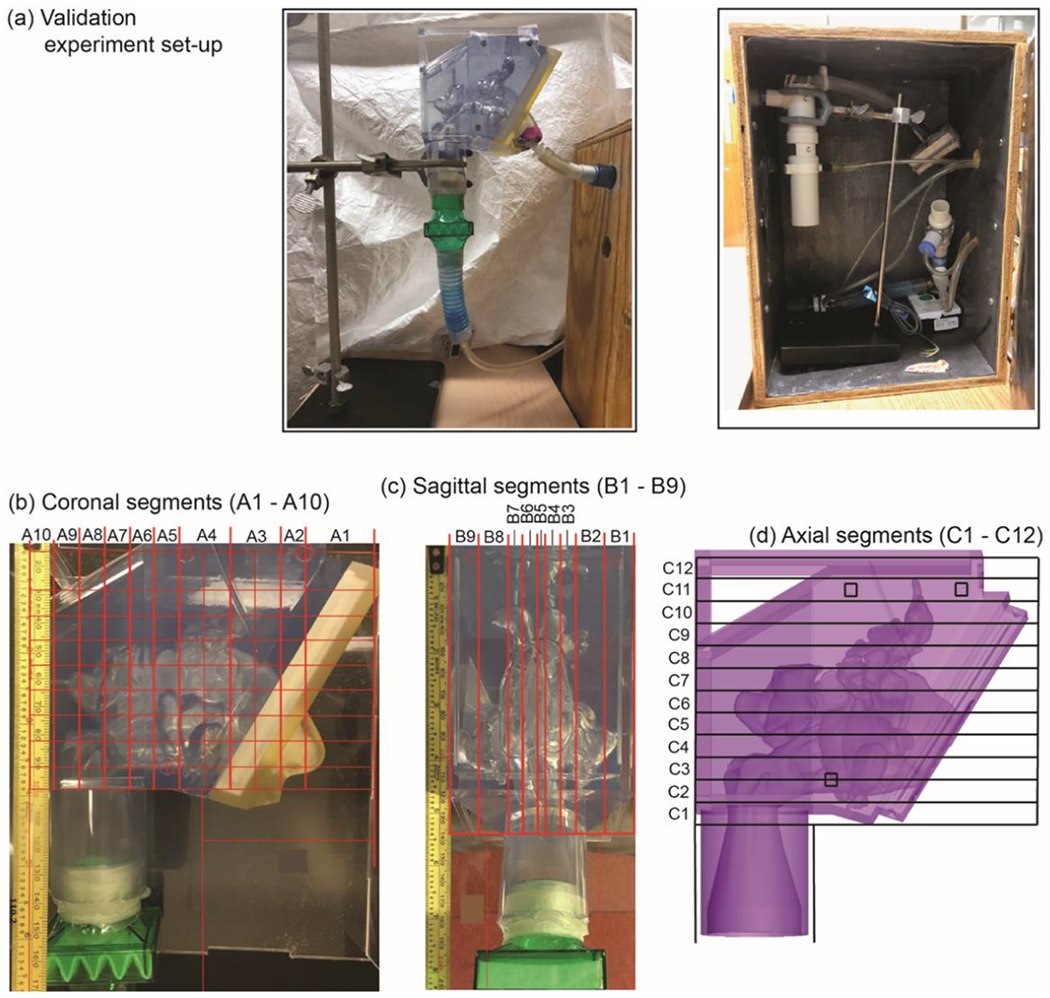
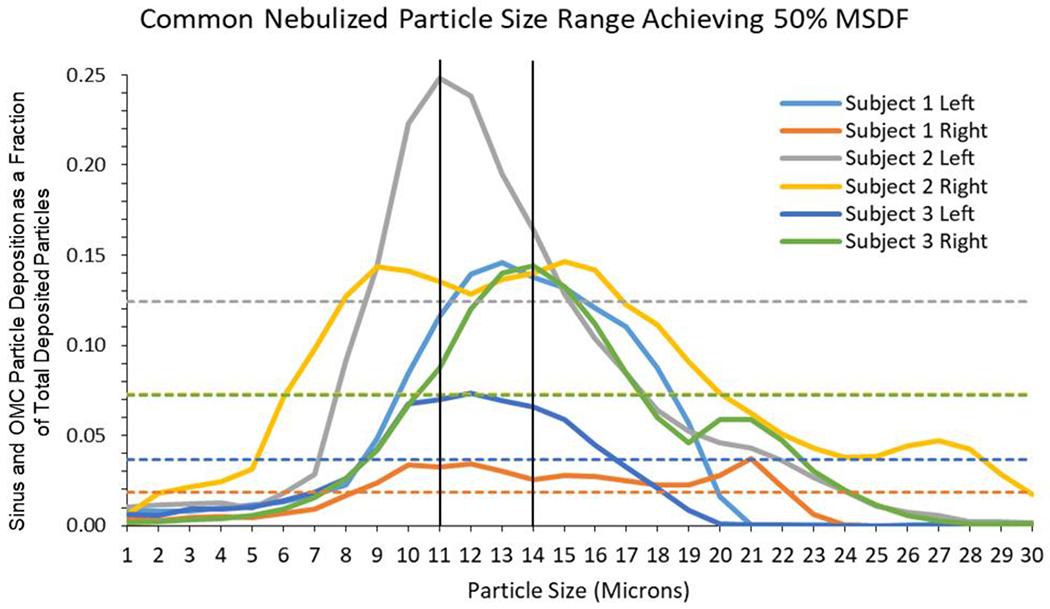
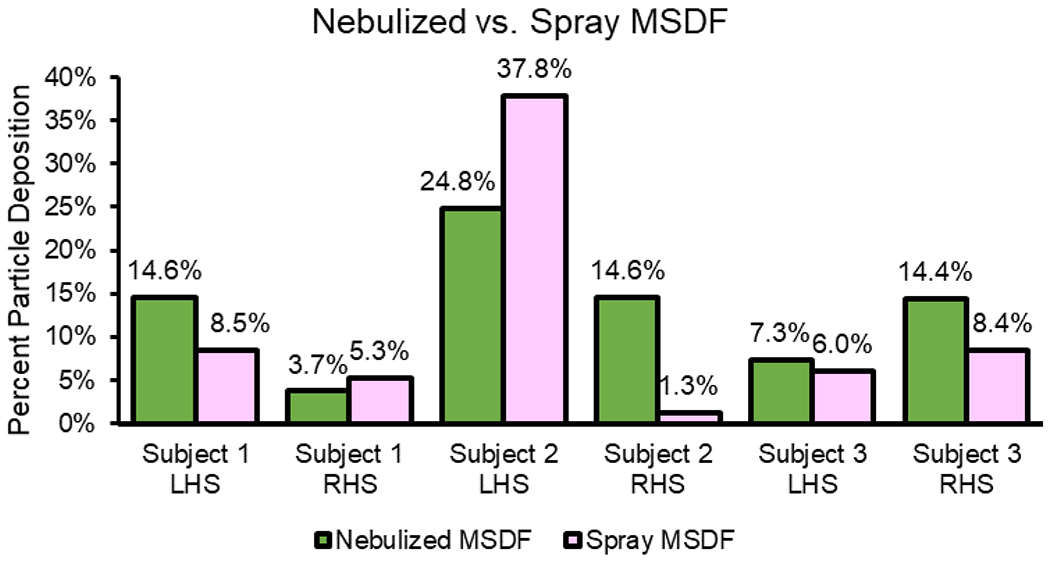
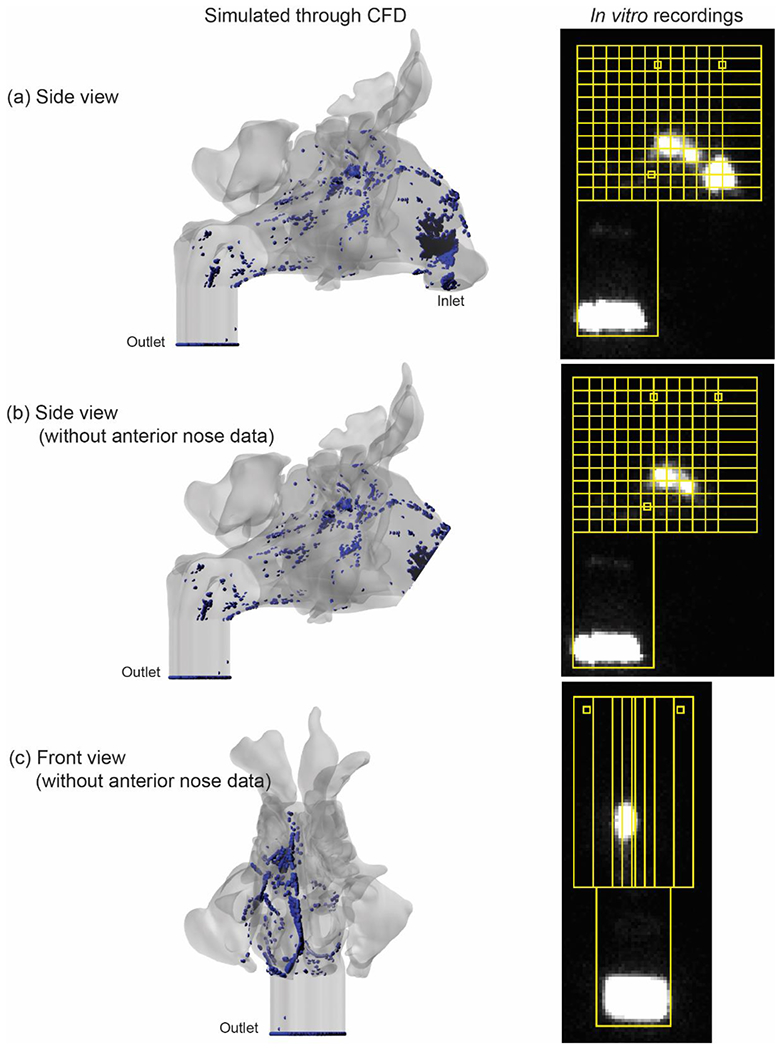
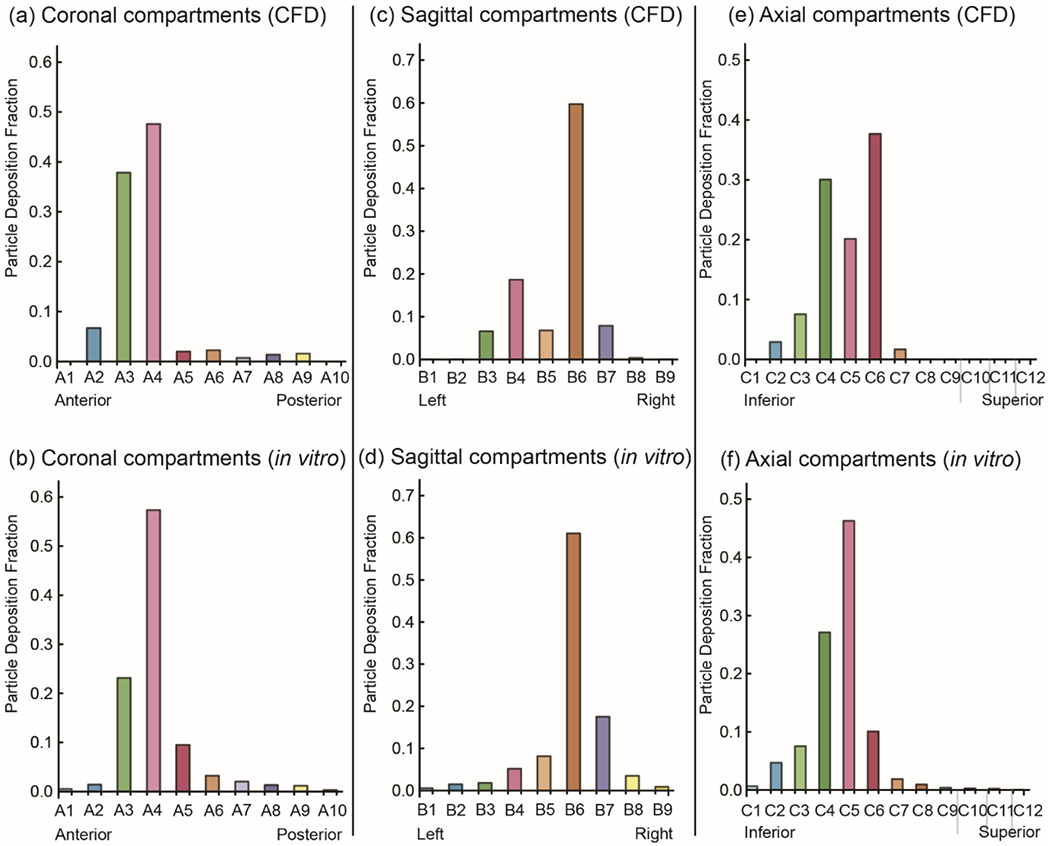
Methods: Three-dimensional models of sinonasal cavities were constructed from computed tomography (CT) scans of 3 subjects with CRS refractory to medical therapy using imaging software. Assuming steady-state inspiratory airflow at resting rate, CFD was used to simulate 1-µm to 120-µm sprayed droplet deposition in the left and right sinuses and OMC with spray nozzle positioning as in current nasal spray use instructions. Zero-velocity nebulization simulations were performed for 1-µm to 30-µm droplet sizes, maximal sinus and OMC deposition fractions (MSDF) were obtained, and sizes that achieved at least 50% of MSDF were identified. Nebulized MSDF was compared to sprayed droplet deposition. We also validated CFD framework through in vitro experiments.
Results: Among nebulized droplet sizes, 11-µm to 14-µm droplets achieved at least 50% of MSDF in all 6 sinonasal cavities. Four of 6 sinonasal cavities had greater sinus and OMC deposition with nebulized droplets than with sprayed droplets at optimal sizes.
Conclusion: Nebulized droplets may target the sinuses and OMC more effectively than sprayed particles at sizes achieving best deposition. Further studies are needed to confirm our preliminary findings. Several commercial nasal nebulizers have average particle sizes outside the optimal nebulized droplet size range found here, suggesting potential for product enhancement.
Keywords: chronic rhinosinusitis; computational fluid dynamics; intranasal steroids; nebulizer; topical drug delivery.
© 2019 ARS-AAOA, LLC.
Conflict of interest statement
Financial Conflict of Interest Disclosure: None
Figures




References
-
- DeConde AS, Soler ZM. Chronic rhinosinusitis: Epidemiology and burden of disease. Am J Rhinol Allergy 2016; 30:134–139 PubMed. - PubMed
-
- Smith KA, Orlandi RR, Rudmik L. Cost of adult chronic rhinosinusitis: A systematic review. Laryngoscope 2015; 125:1547–1556 PubMed. - PubMed
-
- Rudmik L, Smith TL. Quality of life in patients with chronic rhinosinusitis. Curr Allergy Asthma Rep 2011; 11:247–252. - PubMed
-
- Rudmik L, Hoy M, Schlosser RJ et al. Topical therapies in the management of chronic rhinosinusitis: an evidence-based review with recommendations. Int Forum Allergy Rhinol 2013; 3:281–298. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
