

Prenatal diagnosis and management of congenital complete heart block
- PMID: 30821931
- PMCID: PMC6474813
- DOI: 10.1002/bdr2.1459
Prenatal diagnosis and management of congenital complete heart block
Abstract
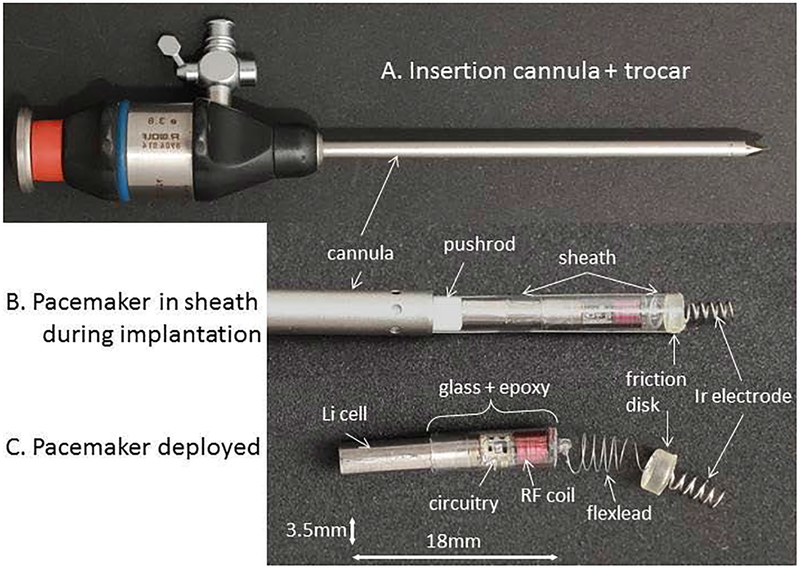
Congenital complete heart block (CCHB) is a life-threatening medical condition in the unborn fetus with insufficiently validated prenatal interventions. Maternal administration of medications aimed at decreasing the immune response in the fetus and beta-agonists intended to increase fetal cardiac output have shown only marginal benefits. Anti-inflammatory therapies cannot reverse CCHB, but may decrease myocarditis and improve heart function. Advances in prenatal diagnosis and use of strict surveillance protocols for delivery timing have demonstrated small improvements in morbidity and mortality. Ambulatory surveillance programs and wearable fetal heart rate monitors may afford early identification of evolving fetal heart block allowing for emergent treatment. There is also preliminary data suggesting a roll for prevention of CCHB with hydroxychloroquine, but the efficacy and safety is still being studied. To date, intrauterine fetal pacing has not been successful due to the high-risk invasive placement techniques and potential problems with lead dislodgement. The development of a fully implantable micropacemaker via a minimally invasive approach has the potential to pace fetal patients with CCHB and thus delay delivery and allow fetal hydrops to resolve. The challenge remains to establish accepted prenatal interventions capable of successfully managing CCHB in utero until postnatal pacemaker placement is successfully achieved.
Keywords: complete heart block; congenital heart block; electro-physiology; fetal cardiology; fetal echocardiography; fetal intervention; pacemakers; prenatal diagnosis.
© 2019 Wiley Periodicals, Inc.
Figures
References
-
- Assad RS, Zielinsky P, Kalil R, Lima G, Aramayo A, Santos A, … Oliveira SA (2003). New lead for in utero pacing for fetal congenital heart block. J Thorac Cardiovasc Surg, 126(1), 300–302. - PubMed
-
- Baruteau AE, Behaghel A, Fouchard S, Mabo P, Schott JJ, Dina C, … Probst V (2012). Parental electrocardiographic screening identifies a high degree of inheritance for congenital and childhood nonimmune isolated atrioventricular block. Circulation, 126(12), 1469–1477. doi: 10.1161/CIRCULATIONAHA.111.069161 - DOI - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
