

Sex Differences in Veterans Admitted to the Hospital for Chronic Obstructive Pulmonary Disease Exacerbation
- PMID: 30822098
- PMCID: PMC6543475
- DOI: 10.1513/AnnalsATS.201809-615OC
Sex Differences in Veterans Admitted to the Hospital for Chronic Obstructive Pulmonary Disease Exacerbation
Abstract
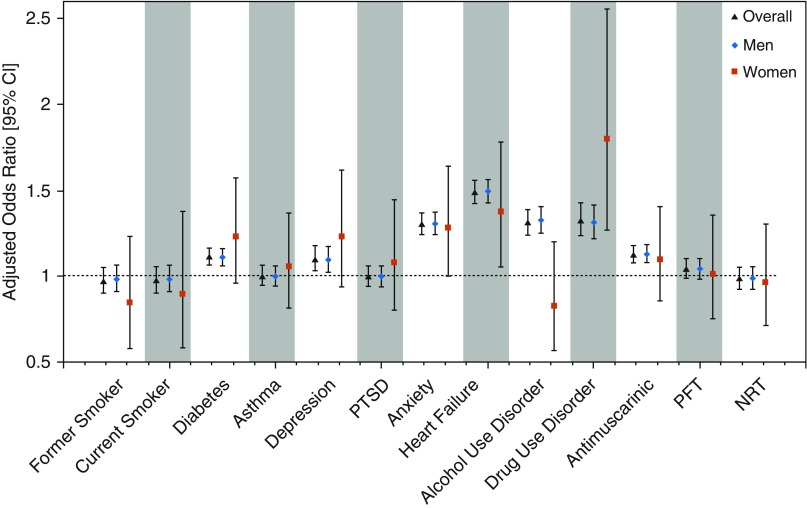
Rationale: As chronic obstructive pulmonary disease (COPD) prevalence in women has outpaced that in men, COPD-related hospitalization and mortality are now higher in women. Presentation, evaluation, and treatment of COPD differ between women and men. Despite higher smoking rates in Veterans, little work has characterized differences in Veterans with COPD by sex. Objectives: To determine risk factors for 30-day readmission among Veterans hospitalized for COPD exacerbations and how they differed by sex. Methods: We performed a retrospective observational analysis of Veterans receiving primary care in Veterans Health Affairs facilities. We included Veterans Administration-based hospitalizations for Veterans with a COPD exacerbation (identified by International Classification of Disease, Ninth Revision codes) who survived to discharge between fiscal years 2012 and 2015. Primary outcome was 30-day readmission. Predictors ascertained before hospitalization included smoking status (current, former, never), pulmonary function testing, pulmonary medication prescriptions, and medical and psychiatric comorbidities (identified by International Classification of Disease, ninth revision codes). We created combined and sex-stratified multivariate logistic regression models to identify associations with 30-day readmission. Results: Our sample included 48,888 Veterans (4% women). Compared with men, women Veterans were younger, more likely to be nonwhite, and differed in smoking status. Women were more likely to have asthma, drug use, and several psychiatric comorbidities. Before hospitalization, women were less likely to have pulmonary function testing (76% vs. 78%; P = 0.01) or be treated with antimuscarinic (43% vs. 48%) or combined long-acting bronchodilator/inhaled corticosteroid (61% vs. 64%) inhalers. Women were more likely to receive nicotine-replacement therapy (all P < 0.01). Women had shorter length of stay (median days, 2 vs. 3; P = 0.04) and lower 30-day readmission rate (20% vs. 22%; P = 0.01). In adjusted models including both sexes, age, antimuscarinic use, comorbidities, and diagnosis of drug or alcohol use were associated with readmission; there was no association with sex and readmission risk. In models stratified by sex, associations were similar between women and men. Conclusions: This study suggests differences between women and men hospitalized for COPD regarding presentation, evaluation, and management. Readmission is strongly influenced by comorbidities, suggesting individualized and comprehensive case management may reduce readmission risk for women and men with COPD.
Keywords: chronic obstructive pulmonary disease; exacerbation; gender; readmission; sex.
Figures
Similar articles
-
Underutilization of Pulmonary Function Testing in Veterans Hospitalized for Chronic Obstructive Pulmonary Disease Exacerbation: Who are We Missing?COPD. 2020 Feb;17(1):15-21. doi: 10.1080/15412555.2019.1711036. Epub 2020 Jan 17. COPD. 2020. PMID: 31948267
-
Depression Is Associated with Readmission for Acute Exacerbation of Chronic Obstructive Pulmonary Disease.Ann Am Thorac Soc. 2016 Feb;13(2):197-203. doi: 10.1513/AnnalsATS.201507-439OC. Ann Am Thorac Soc. 2016. PMID: 26599286 Free PMC article.
-
Reduction in Hospital Readmission Rates Among Medicare Beneficiaries With Chronic Obstructive Pulmonary Disease: A Real-world Outcomes Study of Nebulized Bronchodilators.Clin Ther. 2019 Nov;41(11):2283-2296. doi: 10.1016/j.clinthera.2019.09.001. Epub 2019 Oct 17. Clin Ther. 2019. PMID: 31630815
-
Chronic obstructive pulmonary disease: Useful medications for patients with recurrent symptoms.Prescrire Int. 2016 Nov;25(176):272-277. Prescrire Int. 2016. PMID: 30715829 Review.
-
Exacerbation rate, health status and mortality in COPD--a review of potential interventions.Int J Chron Obstruct Pulmon Dis. 2009;4:203-23. doi: 10.2147/copd.s3385. Epub 2009 Jun 11. Int J Chron Obstruct Pulmon Dis. 2009. PMID: 19554195 Free PMC article. Review.
Cited by
-
Sex-specific differences in physical health and health services use among Canadian Veterans: a retrospective cohort study using healthcare administrative data.BMJ Mil Health. 2023 Oct;169(5):430-435. doi: 10.1136/bmjmilitary-2021-001915. Epub 2021 Oct 11. BMJ Mil Health. 2023. PMID: 34635494 Free PMC article.
-
Characteristics Associated with Spirometry Guideline Adherence in VA Patients Hospitalized with Chronic Obstructive Pulmonary Disease.J Gen Intern Med. 2023 Feb;38(3):619-626. doi: 10.1007/s11606-022-07826-5. Epub 2022 Oct 14. J Gen Intern Med. 2023. PMID: 36241942 Free PMC article.
-
Sex Differences in the Incidence and Outcomes of Patients Hospitalized by Idiopathic Pulmonary Fibrosis (IPF) in Spain from 2016 to 2019.J Clin Med. 2021 Aug 6;10(16):3474. doi: 10.3390/jcm10163474. J Clin Med. 2021. PMID: 34441772 Free PMC article.
-
Association of GLP-1 Receptor Agonists with Chronic Obstructive Pulmonary Disease Exacerbations among Patients with Type 2 Diabetes.Am J Respir Crit Care Med. 2023 Nov 15;208(10):1088-1100. doi: 10.1164/rccm.202303-0491OC. Am J Respir Crit Care Med. 2023. PMID: 37647574 Free PMC article.
-
Prognostic risk factors for moderate-to-severe exacerbations in patients with chronic obstructive pulmonary disease: a systematic literature review.Respir Res. 2022 Aug 23;23(1):213. doi: 10.1186/s12931-022-02123-5. Respir Res. 2022. PMID: 35999538 Free PMC article.
References
-
- Jenkins CR, Chapman KR, Donohue JF, Roche N, Tsiligianni I, Han MK. Improving the management of COPD in women. Chest. 2017;151:686–696. - PubMed
-
- Goel K, Bailey M, Borgstrom M, Parthasarathy S, Natt B, Berry C, et al. Trends in COPD hospitalization and in-hospital deaths in the United States by sex: 2005-2014. Ann Am Thorac Soc. 2018;16:391–393. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
