

Differences in pulmonary arterial flow hemodynamics between children and adults with pulmonary arterial hypertension as assessed by 4D-flow CMR studies
- PMID: 30822118
- PMCID: PMC7327229
- DOI: 10.1152/ajpheart.00802.2018
Differences in pulmonary arterial flow hemodynamics between children and adults with pulmonary arterial hypertension as assessed by 4D-flow CMR studies
Abstract
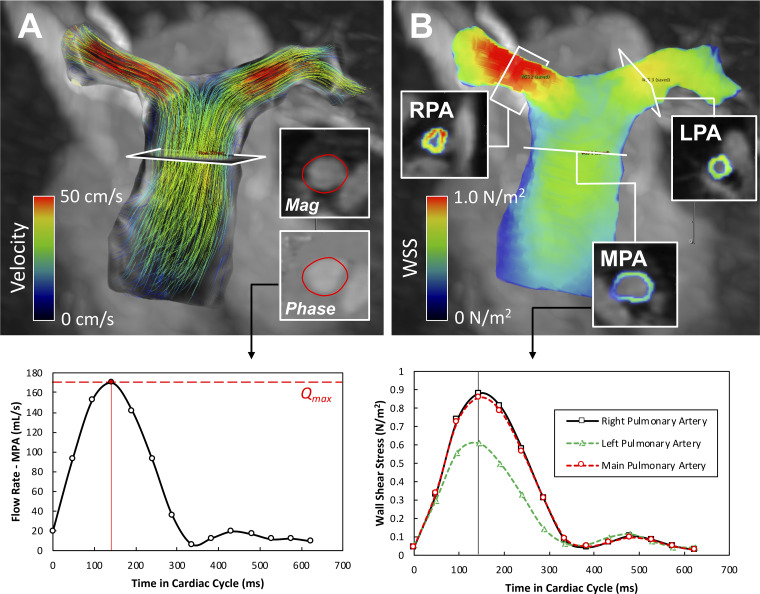
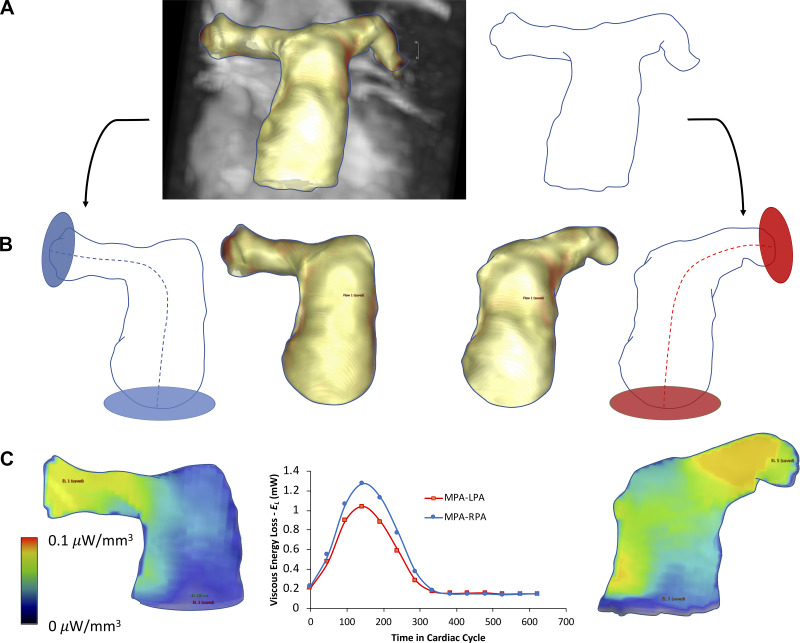
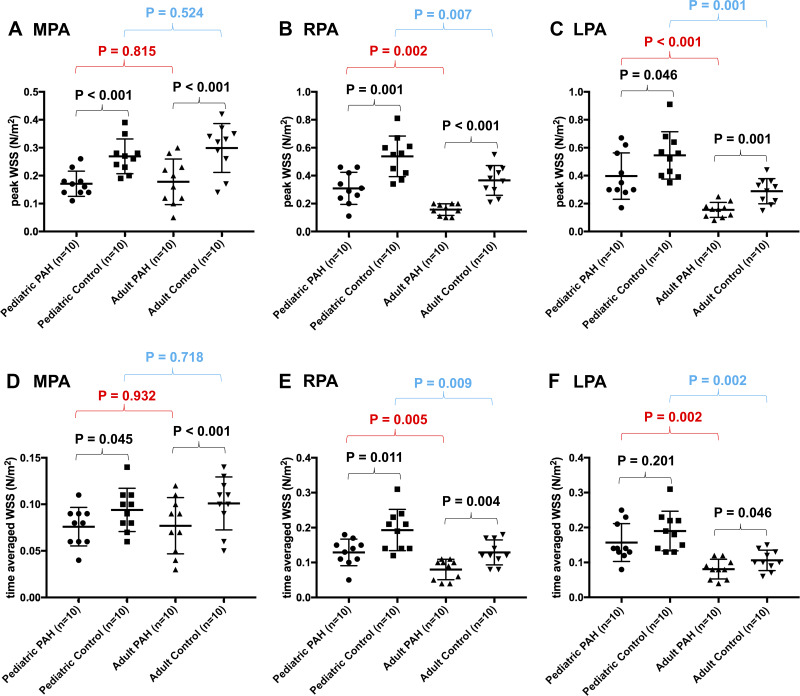
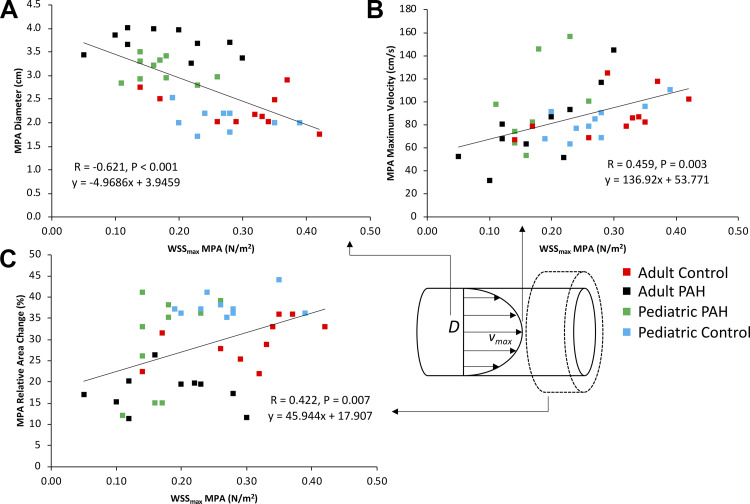
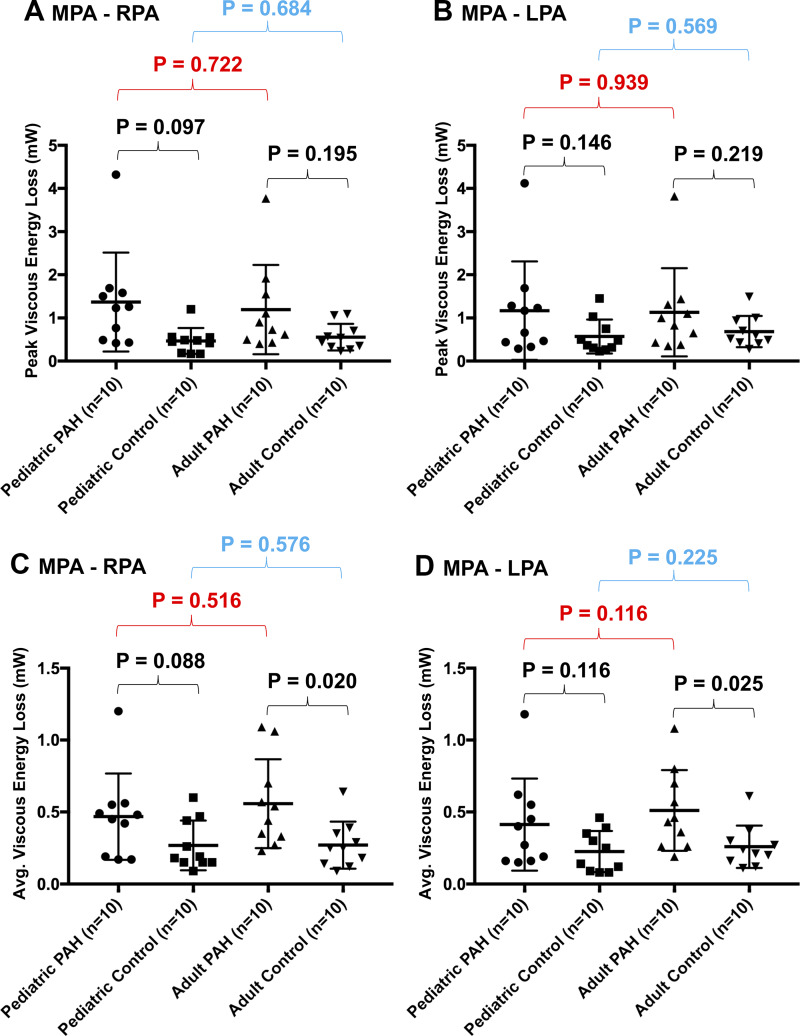
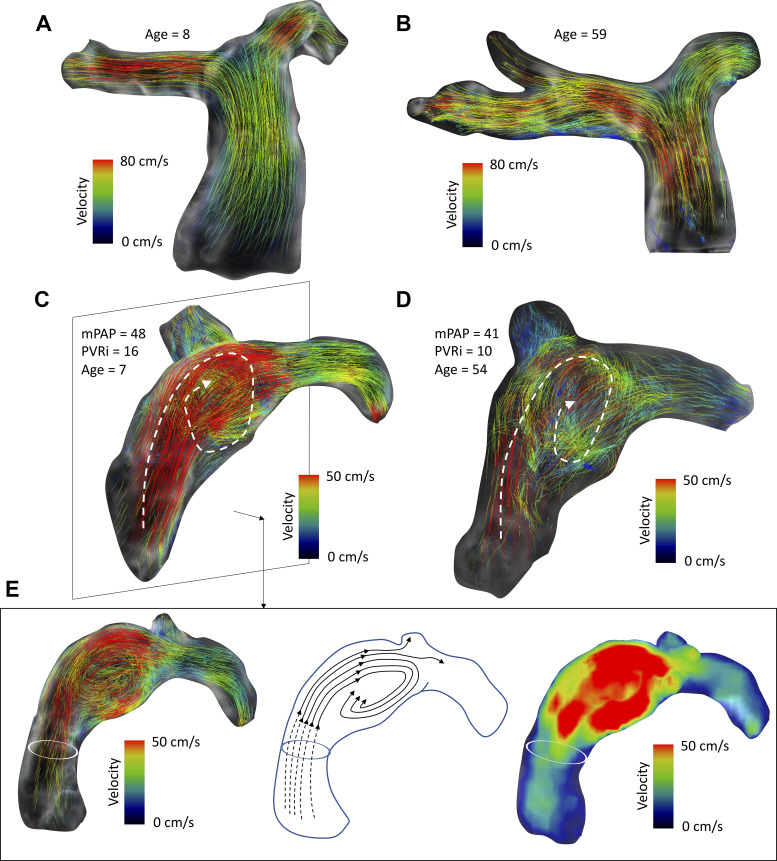
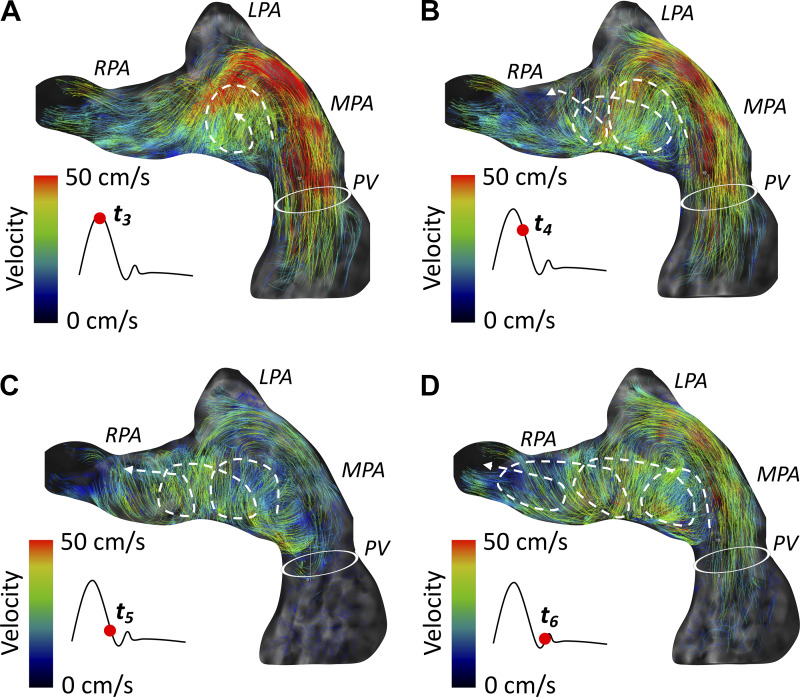
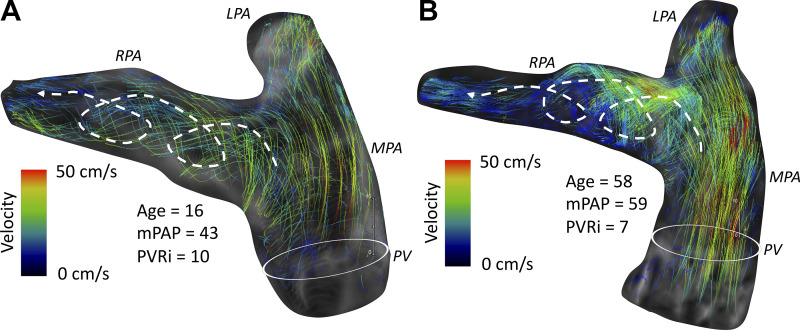
Despite different developmental and pathological processes affecting lung vascular remodeling in both patient populations, differences in 4D MRI findings between children and adults with PAH have not been studied. The purpose of this study was to compare flow hemodynamic state, including flow-mediated shear forces, between pediatric and adult patients with PAH matched by severity of pulmonary vascular resistance index (PVRi). Adults (n = 10) and children (n = 10) with PAH matched by pulmonary vascular resistance index (PVRi) and healthy adult (n = 10) and pediatric (n = 10) subjects underwent comprehensive 4D-flow MRI to assess peak systolic wall shear stress (WSSmax) measured in the main (MPA), right (RPA), and left pulmonary arteries (LPA), viscous energy loss (EL) along the MPA-RPA and MPA-LPA tract, and qualitative analysis of secondary flow hemodynamics. WSSmax was decreased in all pulmonary vessels in children with PAH when compared with the same age group (all P < 0.05). Similarly, WSSmax was decreased in all pulmonary vessels in adult PAH patients when compared with healthy adult subjects (all P < 0.01). Average EL was increased in adult patients with PAH when compared with the same age group along both MPA-RPA (P = 0.020) and MPA-LPA (P = 0.025) tracts. There were no differences in EL indices between adults and pediatric patients. Children and adult patients with PAH have decreased shear hemodynamic forces. However, pathological flow hemodynamic formations appear to be more consistent in adult patients, whereas flow hemodynamic abnormalities appear to be more variable in children with PAH for comparable severity of PVRi. NEW & NOTEWORTHY Both children and adult patients with PAH have decreased shear hemodynamic forces inside the pulmonary arteries associated with the degree of vessel dilation and stiffness. These differences also exist between healthy normotensive children and adults. However, pathological flow hemodynamic formations appear to more uniform in adult patients, whereas in children with PAH flow, hemodynamic abnormalities appear to be more variable. Pathological flow formations appear not to have a major effect on viscous energy loss associated with the flow conduction through proximal pulmonary arteries.
Keywords: cardiac magnetic resonance; flow; magnetic resonance imaging; pediatric and adult; pulmonary arterial hypertension.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
Similar articles
-
3D Vortex-Energetics in the Left Pulmonary Artery for Differentiating Pulmonary Arterial Hypertension and Pulmonary Venous Hypertension Groups Using 4D Flow MRI.J Magn Reson Imaging. 2025 May;61(5):2130-2143. doi: 10.1002/jmri.29635. Epub 2024 Oct 28. J Magn Reson Imaging. 2025. PMID: 39467263 Free PMC article.
-
Non-invasive assessment of cardiac function and pulmonary vascular resistance in an canine model of acute thromboembolic pulmonary hypertension using 4D flow cardiovascular magnetic resonance.J Cardiovasc Magn Reson. 2014 Mar 13;16(1):23. doi: 10.1186/1532-429X-16-23. J Cardiovasc Magn Reson. 2014. PMID: 24625242 Free PMC article.
-
Hemodynamics assessment using 4D flow CMR before and after balloon pulmonary angioplasty in chronic thromboembolic pulmonary hypertension: a retrospective observational study.BMC Cardiovasc Disord. 2025 Aug 21;25(1):621. doi: 10.1186/s12872-025-05068-x. BMC Cardiovasc Disord. 2025. PMID: 40841600 Free PMC article.
-
Clinical Application of 4D Flow MR Imaging to Pulmonary Hypertension.Magn Reson Med Sci. 2022 Mar 1;21(2):309-318. doi: 10.2463/mrms.rev.2021-0111. Epub 2022 Feb 19. Magn Reson Med Sci. 2022. PMID: 35185084 Free PMC article. Review.
-
MR and CT Imaging for the Evaluation of Pulmonary Hypertension.JACC Cardiovasc Imaging. 2016 Jun;9(6):715-32. doi: 10.1016/j.jcmg.2015.12.015. JACC Cardiovasc Imaging. 2016. PMID: 27282439 Free PMC article. Review.
Cited by
-
Interactive effect of hemodynamics in transverse sigmoid sinus and bone morphology on venous pulsatile tinnitus: a four-dimensional (4D) flow magnetic resonance imaging (MRI) study.Quant Imaging Med Surg. 2024 Sep 1;14(9):6647-6659. doi: 10.21037/qims-24-610. Epub 2024 Aug 21. Quant Imaging Med Surg. 2024. PMID: 39281126 Free PMC article.
-
Multicenter research priorities in pediatric CMR: results of a collaborative wiki survey.Sci Rep. 2023 Jun 3;13(1):9022. doi: 10.1038/s41598-023-34720-9. Sci Rep. 2023. PMID: 37270629 Free PMC article.
-
Patient-Specific Inverse Modeling of In Vivo Cardiovascular Mechanics with Medical Image-Derived Kinematics as Input Data: Concepts, Methods, and Applications.Appl Sci (Basel). 2022 Apr 2;12(8):3954. doi: 10.3390/app12083954. Epub 2022 Apr 14. Appl Sci (Basel). 2022. PMID: 36911244 Free PMC article.
-
Physiological shear stress suppresses apoptosis in human pulmonary microvascular endothelial cells.Physiol Rep. 2025 Mar;13(6):e70269. doi: 10.14814/phy2.70269. Physiol Rep. 2025. PMID: 40110888 Free PMC article.
-
Role of cardiovascular magnetic resonance in pediatric pulmonary hypertension-novel concepts and imaging biomarkers.Cardiovasc Diagn Ther. 2021 Aug;11(4):1057-1069. doi: 10.21037/cdt-20-270. Cardiovasc Diagn Ther. 2021. PMID: 34527532 Free PMC article. Review.
References
-
- Abman SH, Hansmann G, Archer SL, Ivy DD, Adatia I, Chung WK, Hanna BD, Rosenzweig EB, Raj JU, Cornfield D, Stenmark KR, Steinhorn R, Thébaud B, Fineman JR, Kuehne T, Feinstein JA, Friedberg MK, Earing M, Barst RJ, Keller RL, Kinsella JP, Mullen M, Deterding R, Kulik T, Mallory G, Humpl T, Wessel DL; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia; and the American Thoracic Society . Pediatric pulmonary hypertension: Guidelines from the American Heart Association and American Thoracic Society. Circulation 132: 2037–2099, 2015. [Correction in Circulation 133: e368, 2016.]. doi:10.1161/CIR.0000000000000329. - DOI - PubMed
-
- Barker AJ, Roldán-Alzate A, Entezari P, Shah SJ, Chesler NC, Wieben O, Markl M, François CJ. Four-dimensional flow assessment of pulmonary artery flow and wall shear stress in adult pulmonary arterial hypertension: results from two institutions. Magn Reson Med 73: 1904–1913, 2015. doi:10.1002/mrm.25326. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous