

Flavonoid Mixture Inhibits Mycobacterium tuberculosis Survival and Infectivity
- PMID: 30823377
- PMCID: PMC6429385
- DOI: 10.3390/molecules24050851
Flavonoid Mixture Inhibits Mycobacterium tuberculosis Survival and Infectivity
Abstract
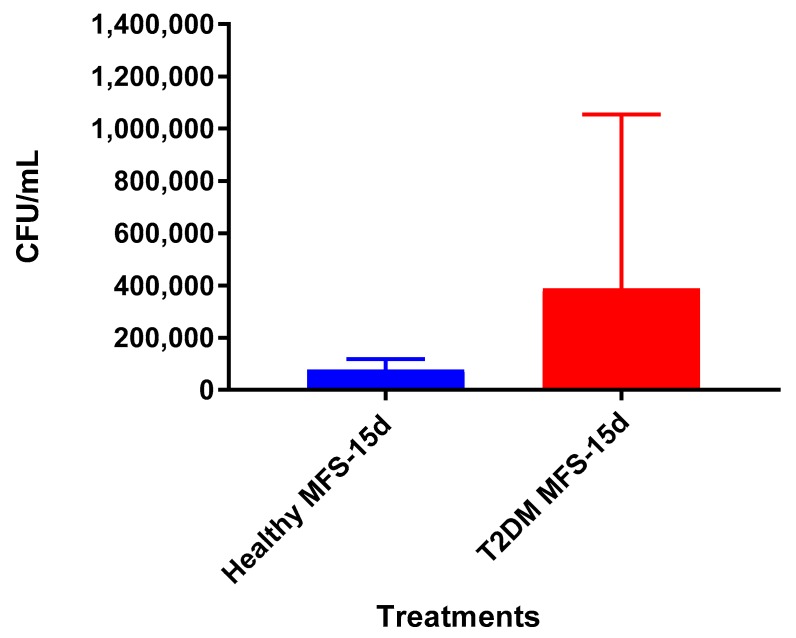
Background: Flavonoids have been shown to exert anti-pathogenic potential, but few studies have investigated their effects on Mycobacterium tuberculosis (Mtb) infectivity. We hypothesized that a flavonoid mixture would have a favorable influence on cell death and the resolution of Mtb infection in THP-1 macrophages and in granulomas derived from both healthy participants and those with type 2 diabetes mellitus (T2DM).
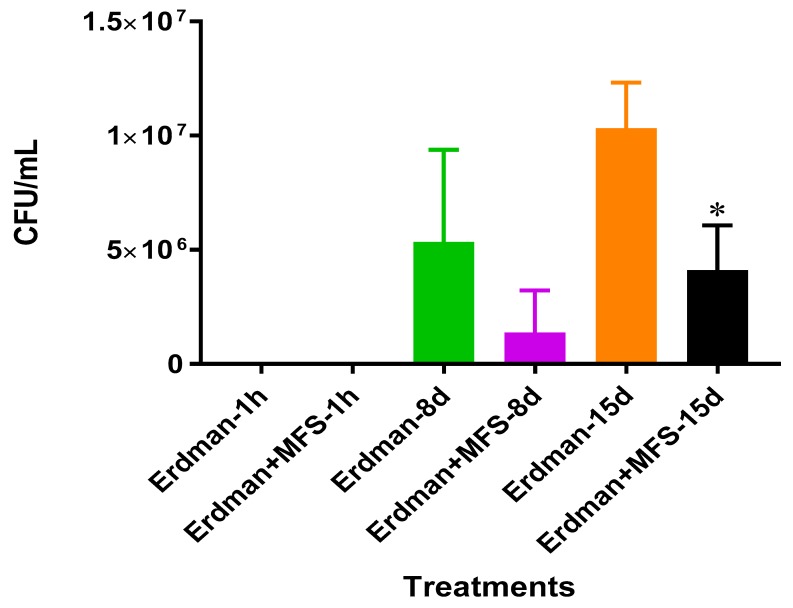
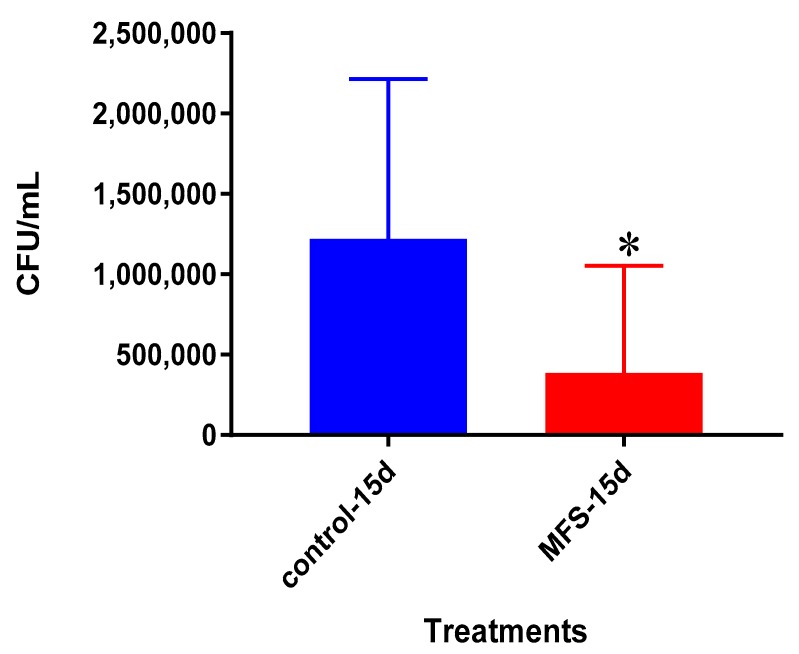
Methods: THP-1 macrophages, and in vitro granulomas from healthy participants (N = 8) and individuals with T2DM (N = 5) were infected with Mtb. A mixed flavonoid supplement (MFS) at a concentration of 0.69 mg per ml was added as treatment to Mtb infected THP-1 macrophages and granulomas for 8 to 15 days.
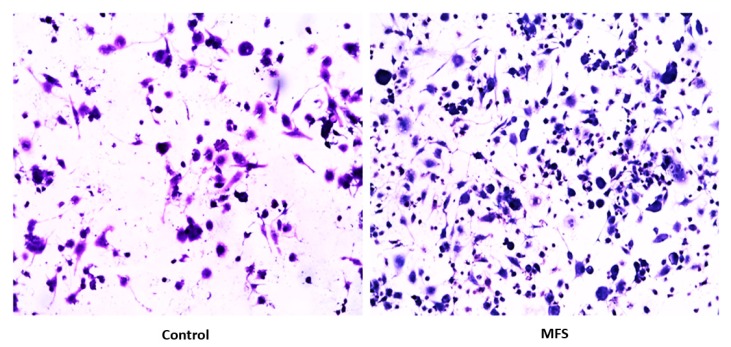
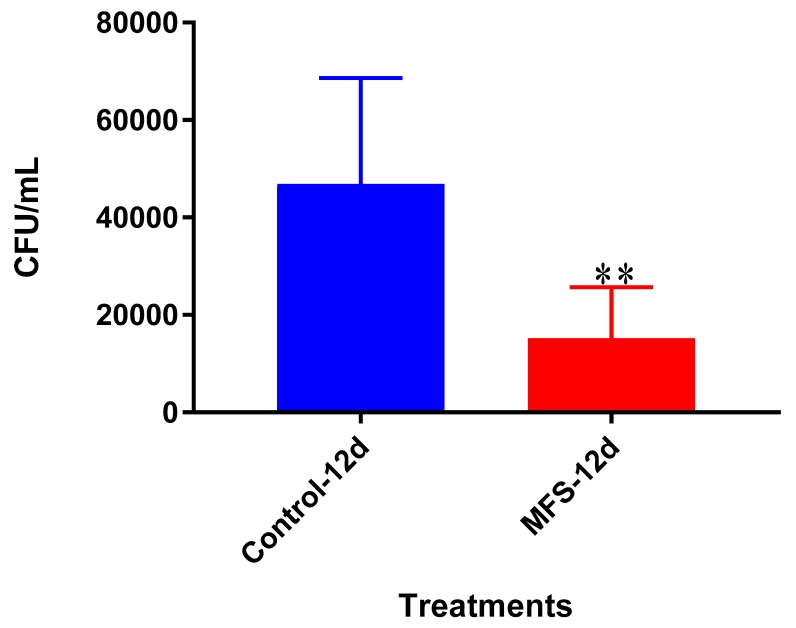
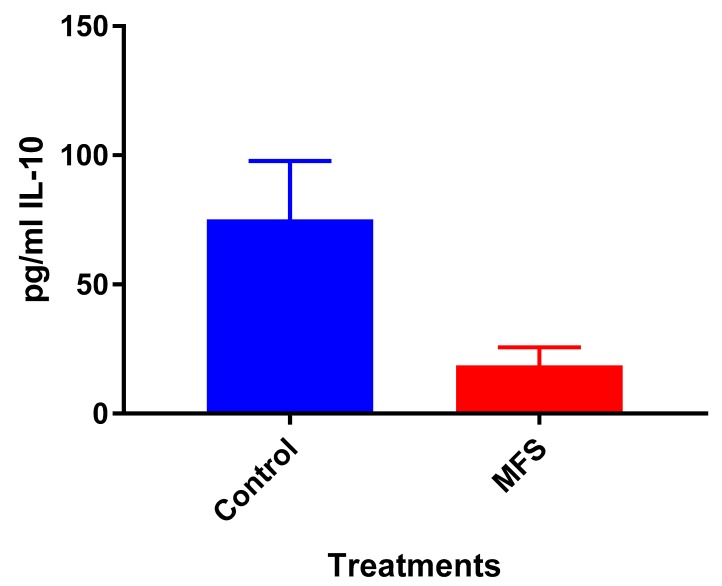
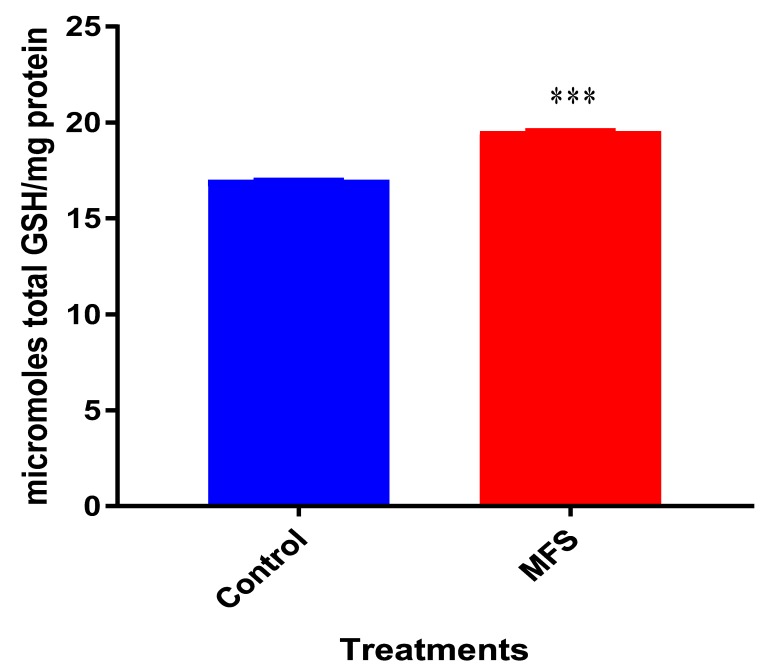
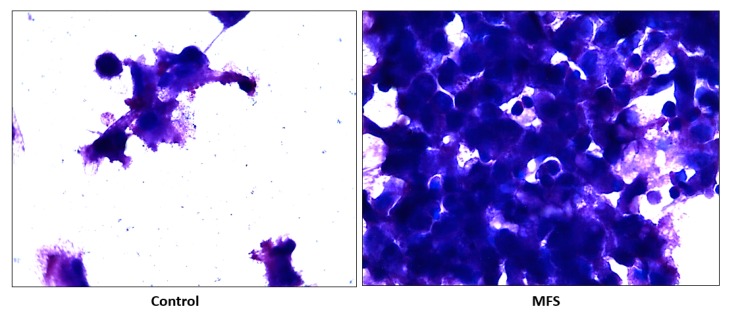
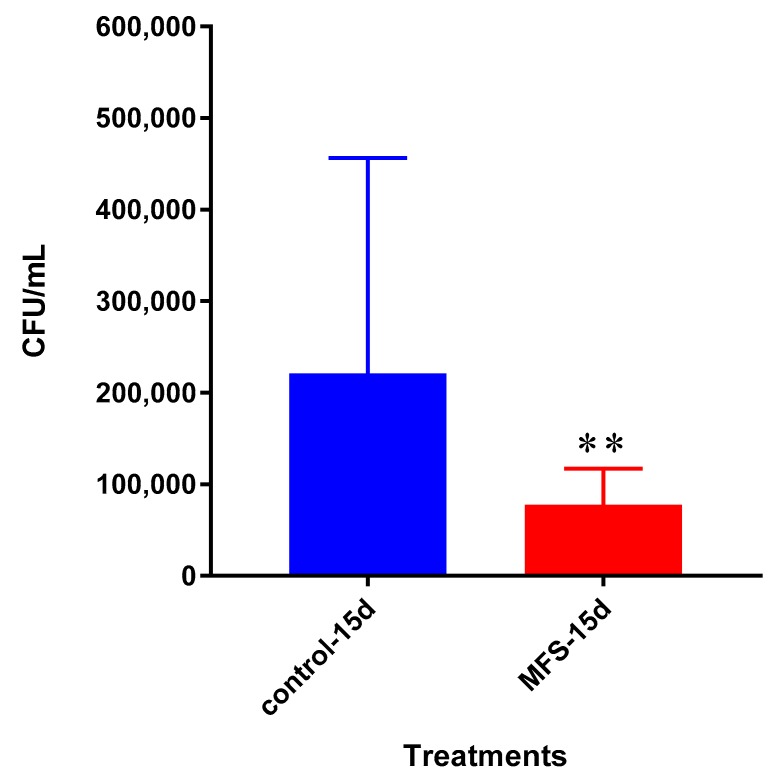
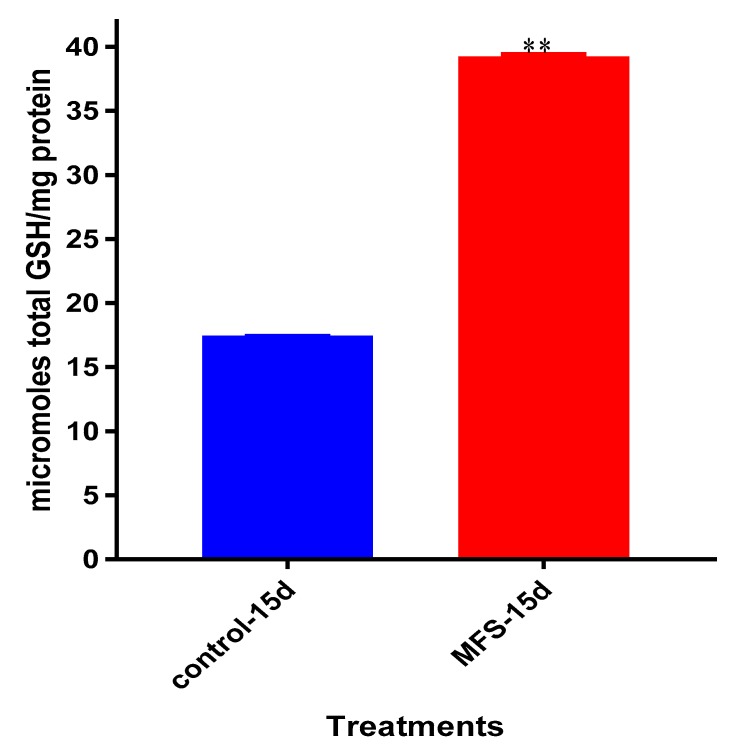
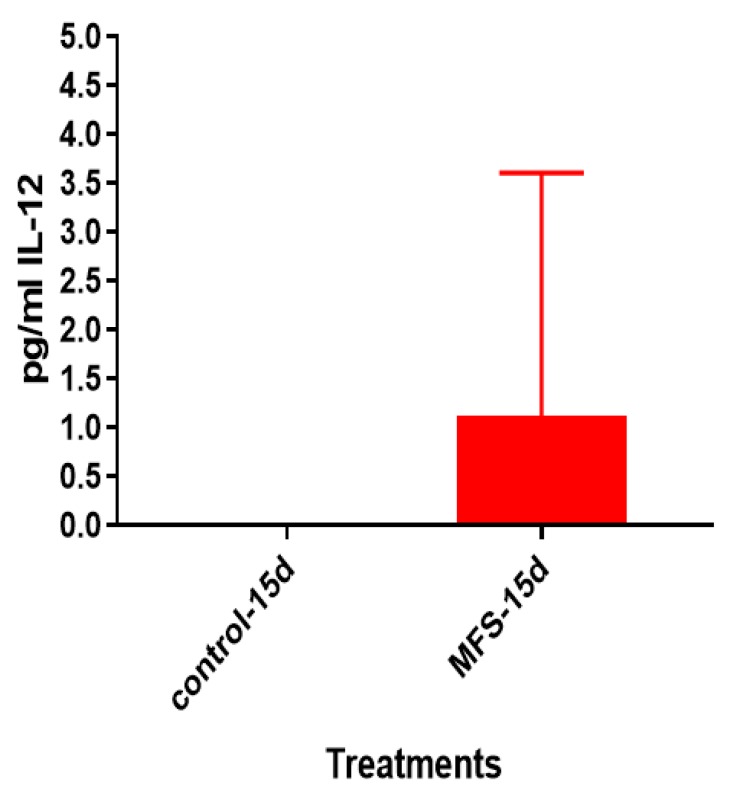
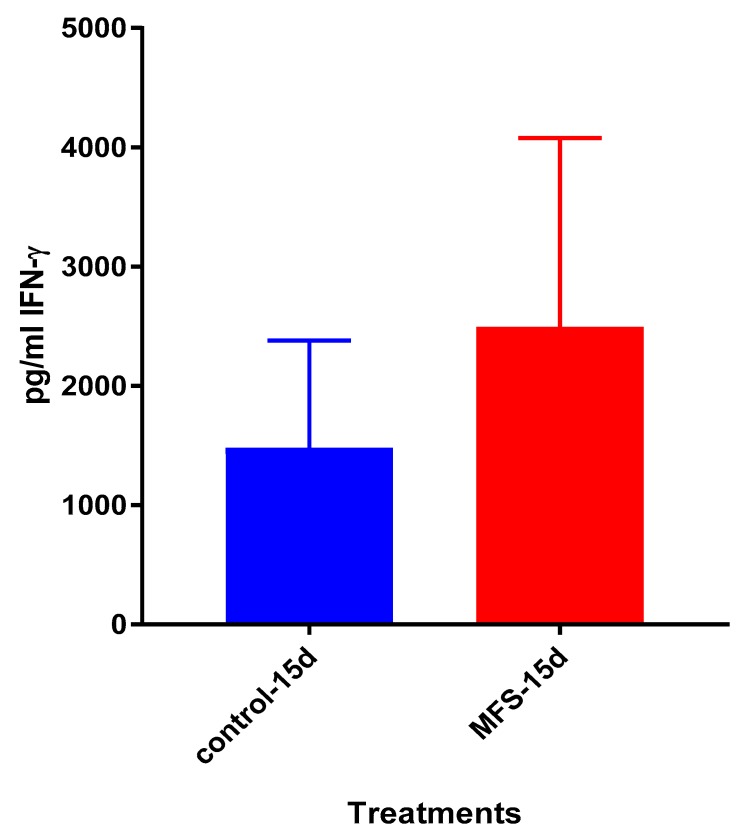
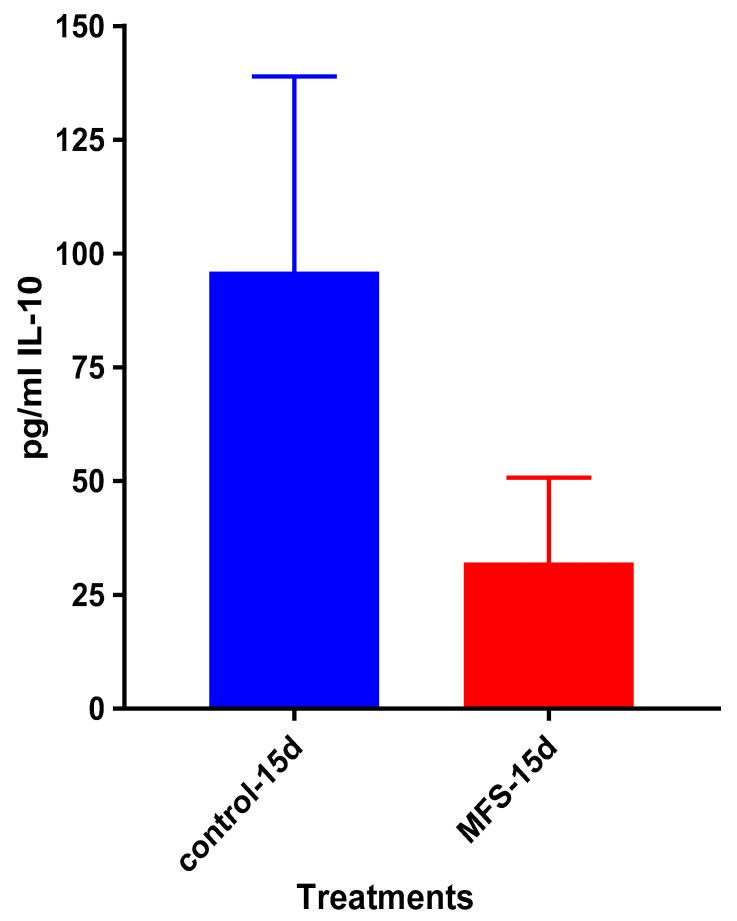
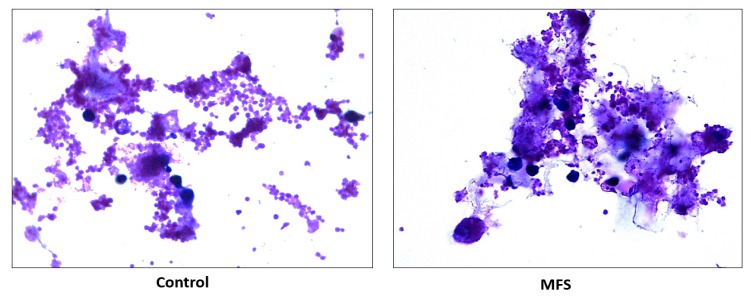
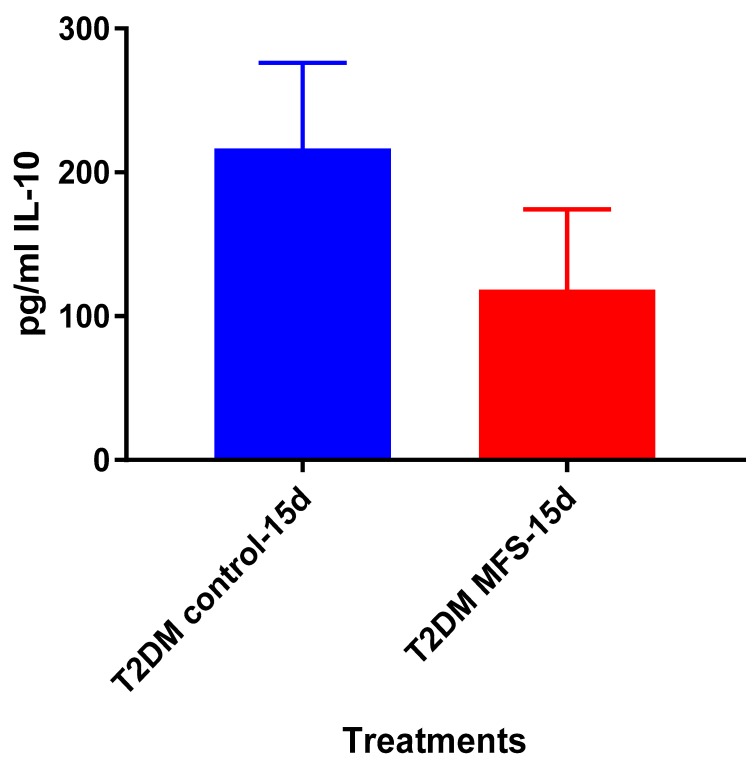
Results: MFS treatment significantly reduced the intracellular Mtb survival, increased cell density, aggregation, and granuloma formation, and increased glutathione (GSH) levels. IL-12 and IFN-γ levels tended to be higher and IL-10 lower when Mtb infected THP-1 macrophages and granulomas obtained from healthy subjects were treated with MFS compared to control.
Conclusions: MFS treatment exerted a strong influence against Mtb infectivity in THP-1 macrophages and in granulomas including antimycobacterial effects, GSH enrichment, cytokine regulation, and augmented granuloma formation. Our data support the strategy of increased flavonoid intake for managing tuberculosis.
Keywords: Mtb; Mycobacterium tuberculosis; T2DM; TB; flavonoids; glutathione; immunomodulation; polyphenols.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- World Health Organization . Global Tuberculosis Report 2015. World Health Organization; Geneva, Switzerland: 2015.
-
- Tacconelli E., Carrara E., Savoldi A., Harbarth S., Mendelson M., Monnet D.L., Pulcini C., Kahlmeter G., Kluytmans J., Carmeli Y., et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet. Infect. Dis. 2018;18:318–327. doi: 10.1016/S1473-3099(17)30753-3. - DOI - PubMed
-
- World Health Organization Diabetes. [(accessed on 30 July 2018)]; Available online: http://www.who.int/news-room/fact-sheets/detail/diabetes.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
