

Fractional flow reserve-guided complete revascularization versus culprit-only revascularization in acute ST-segment elevation myocardial infarction and multi-vessel disease patients: a meta-analysis and systematic review
- PMID: 30823897
- PMCID: PMC6397458
- DOI: 10.1186/s12872-019-1022-6
Fractional flow reserve-guided complete revascularization versus culprit-only revascularization in acute ST-segment elevation myocardial infarction and multi-vessel disease patients: a meta-analysis and systematic review
Abstract
Background: Approximately 30-50% patients with acute ST-segment elevation myocardial infarction (STMEI) were found to have non-infarct-related coronary artery (IRA) disease, which was significantly associated with worse prognosis. However, challenges still remain for these patients: which non-infarct-related lesion should be treated and when should the procedure be performed? The present study aims to investigate Fractional flow reserve (FFR)-guided complete revascularization (CR) in comparison to culprit-only revascularization (COR) in patients with ST-segment elevation myocardial infarction (STEMI) and multi-vessel disease (MVD).
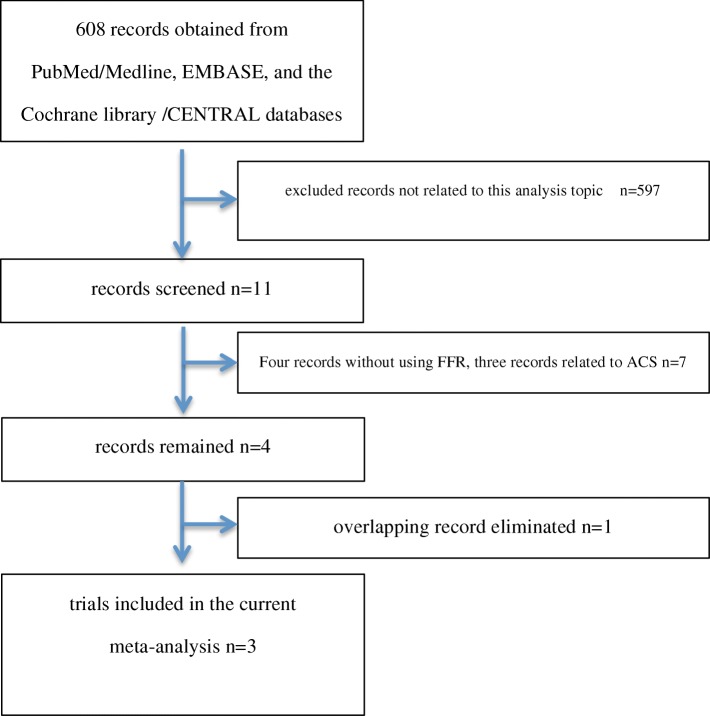
Methods: Three appropriate randomized controlled trials (RCTs) were selected from the PubMed/Medline, EMBASE, and the Cochrane library /CENTRAL databases. 1631 patients (688 patients underwent FFR-guided CR and 943 patients underwent COR) following-up 12-44 months was evaluated.
Results: FFR-guided CR significantly reduced major adverse cardiac event (MACE) (OR 0.47, 95% CI: 0.35-0.62, P < 0.00001) and ischemia-driven repeat revascularization (OR 0.36, 0.26-0.51, P < 0.00001), as compared to COR. However, there is no difference in all-cause mortality (OR 1.24, 0.65-2.35, P = 0.51).
Conclusions: In patients with STEMI and MVD, FFR-guided CR is better than COR in terms of MACE and ischemia-driven repeat revascularization, while there are almost similar in all-cause mortality.
Trial registration: All analyses were based on previous published studies, thus no ethical approval and patient consent are required COMPARE-ACUTE trial number NCT01399736 ; DANAMI-3-PRIMULTI trial number NCT01960933 .
Keywords: Complete revascularization; Culprit-only revascularization; Fractional flow reserve; Multi-vessel disease; ST-segment elevation myocardial infarction.
Conflict of interest statement
Ethics approval and consent to participate
All analyses were based on previous published studies, thus no ethical approval and patient consent are required.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures





References
-
- Shah R, Clare RM, Chiswell K, Jones WS, Kumar AS, Thiele H, Smalling RW, Chandra P, Cohen M, Perera D, Chew DP, French JK, Blaxill J, Ohman EM, Patel MR. Impact of non-infarct-related artery disease on infarct size and outcomes (from the CRISP-AMI trial) Am J Med. 2016;129:1307–1315. doi: 10.1016/j.amjmed.2016.07.011. - DOI - PubMed
-
- Park DW, Clare RM, Schulte PJ, Pieper KS, Shaw LK, Califf RM, Ohman EM, Vande Werf F, Hirji S, Harrington RA, Armstrong PW, Granger CB, Jeong MH, Patel MR. Extent, location, and clinical significance of non-infarct-related coronary artery disease among patients with ST-elevation myocardial infarction. JAMA. 2014;312(19):2019–2027. doi: 10.1001/jama.2014.15095. - DOI - PubMed
-
- Hannan EL, Samadashvili Z, Walford G, Holmes DR, Jacobs AK, Stamato NJ, Venditti FJ, Sharma S, King SB. Culprit vessel percutaneous coronary intervention versus multivessel and staged percutaneous coronary intervention for ST-segment elevation myocardial infarction patients with multivessel disease. J Am Coll Cardiol Intv. 2010;3:22–31. doi: 10.1016/j.jcin.2009.10.017. - DOI - PubMed
-
- Toma M, Buller CE, Westerhout CM, Fu Y, O’Neill WW, Holmes Jr DR, Hamm CW, Granger CB, Paul W, Armstrong, for the APEX-AMI Investigators Non-culprit coronary artery percutaneous coronary intervention during acute ST-segment elevation myocardial infarction: insights from the APEX-AMI trial. Eur Heart J. 2010;31:1701–1707. doi: 10.1093/eurheartj/ehq129. - DOI - PubMed
-
- Vlaar PJ, Mahmoud KD, Holmes DR, Jr, van Valkenhoef G, Hillege HL, van der Horst IC, Zijlstra F, de Smet BJ. Culprit vessel only versus multivessel and staged percutaneous coronary intervention for multivessel disease in patients presenting with ST-segment elevation myocardial infarction: a pairwise and network meta-analysis. J Am Coll Cardiol. 2011;58:692–703. doi: 10.1016/j.jacc.2011.03.046. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
