

Three prophylaxis regimens (tacrolimus, mycophenolate mofetil, and cyclophosphamide; tacrolimus, methotrexate, and bortezomib; or tacrolimus, methotrexate, and maraviroc) versus tacrolimus and methotrexate for prevention of graft-versus-host disease with haemopoietic cell transplantation with reduced-intensity conditioning: a randomised phase 2 trial with a non-randomised contemporaneous control group (BMT CTN 1203)
- PMID: 30824040
- PMCID: PMC6503965
- DOI: 10.1016/S2352-3026(18)30221-7
Three prophylaxis regimens (tacrolimus, mycophenolate mofetil, and cyclophosphamide; tacrolimus, methotrexate, and bortezomib; or tacrolimus, methotrexate, and maraviroc) versus tacrolimus and methotrexate for prevention of graft-versus-host disease with haemopoietic cell transplantation with reduced-intensity conditioning: a randomised phase 2 trial with a non-randomised contemporaneous control group (BMT CTN 1203)
Abstract
Background: Prevention of graft-versus-host disease (GvHD) without malignant relapse is the overall goal of allogeneic haemopoietic cell transplantation (HCT). We aimed to evaluate regimens using either maraviroc, bortezomib, or post-transplantation cyclophosphamide for GvHD prophylaxis compared with controls receiving the combination of tacrolimus and methotrexate using a novel composite primary endpoint to identify the most promising intervention to be further tested in a phase 3 trial.
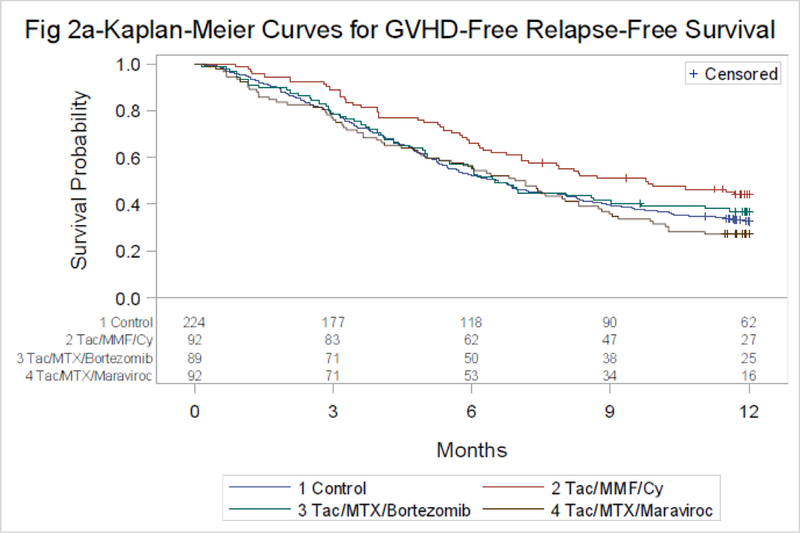
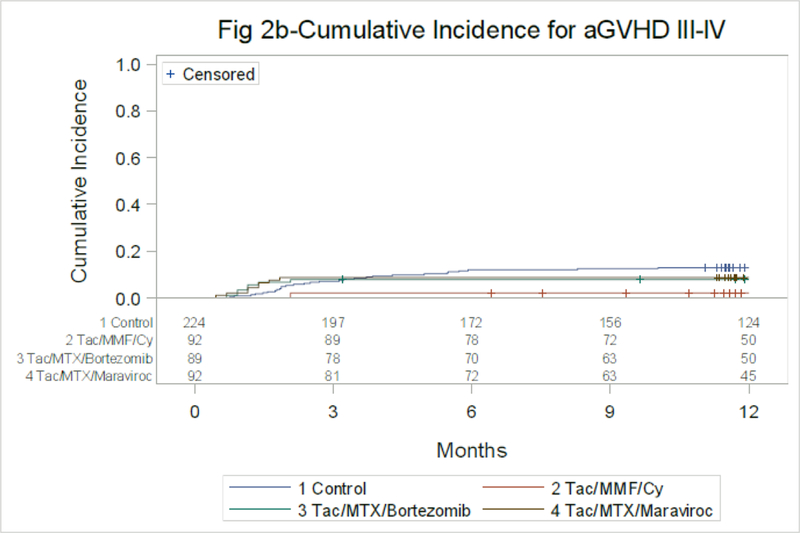
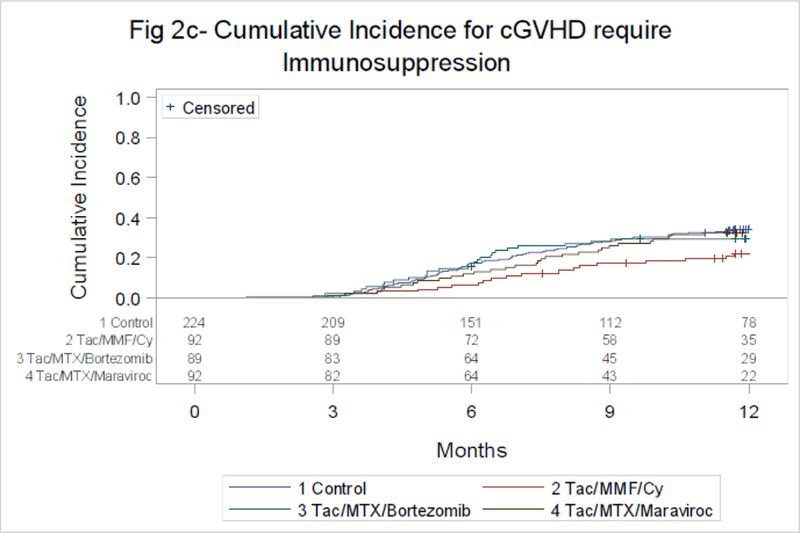
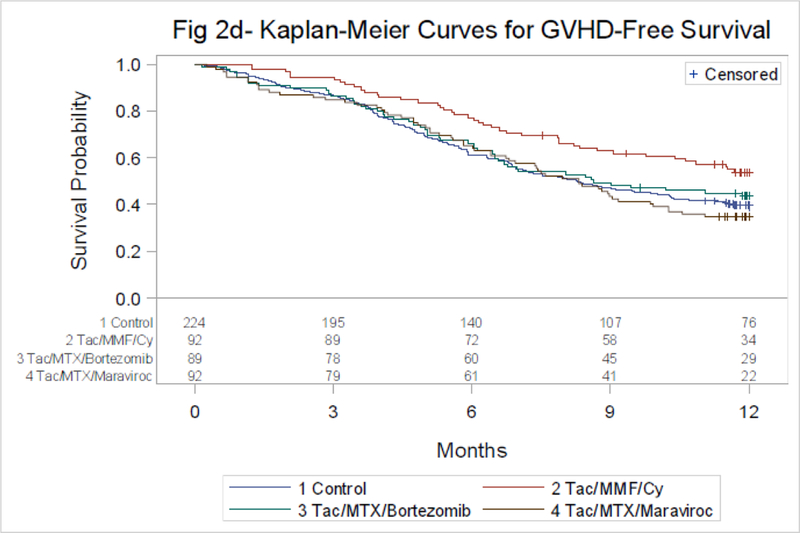
Methods: In this prospective multicentre phase 2 trial, adult patients aged 18-75 years who received reduced-intensity conditioning HCT were randomly assigned (1:1:1) by random block sizes to tacrolimus, mycophenolate mofetil, and post-transplantation cyclophosphamide (cyclophosphamide 50 mg/kg on days 3 and 4, followed by tacrolimus starting on day 5 and mycophenolate mofetil starting on day 5 at 15 mg/kg three times daily not to exceed 1 g from day 5 to day 35); tacrolimus, methotrexate, and bortezomib (bortezomib 1·3 mg/m2 intravenously on days 1, 4, and 7 after HCT); or tacrolimus, methotrexate, and maraviroc (maraviroc 300 mg orally twice daily from day -3 to day 30 after HCT). Methotrexate was administered as a 15 mg/m2 intravenous bolus on day 1 and 10 mg/m2 intravenous bolus on days 3, 6, and 11 after HCT; tacrolimus was given intravenously at a dose of 0·05 mg/kg twice daily (or oral equivalent) starting on day -3 (except the post-transplantation cyclophosphamide, as indicated), with a target level of 5-15 ng/mL. Tacrolimus was continued at least until day 90 and was tapered off by day 180. Each study group was compared separately to a contemporary non-randomised prospective cohort of patients (control group) who fulfilled the same eligibility criteria as the trial, but who were treated with tacrolimus and methotrexate at centres not participating in the trial. The primary endpoint (GvHD-free, relapse-free survival [GRFS]) was defined as the time from HCT to onset of grade 3-4 acute GvHD, chronic GvHD requiring systemic immunosuppression, disease relapse, or death. The study was analysed by modified intention to treat. The study is closed to accrual and this is the planned analysis. This trial is registered with ClinicalTrials.gov, number NCT02208037.
Findings: Between Nov 17, 2014, and May 18, 2016, 273 patients from 31 US centres were randomly assigned to the three study arms: 89 to tacrolimus, methotrexate, and bortezomib; 92 to tacrolimus, methotrexate, and maraviroc; 92 to tacrolimus, mycophenolate mofetil, and post-transplantation cyclophosphamide; and six were excluded. Between Aug 1, 2014, and Sept 14, 2016, 224 controls received tacrolimus and methotrexate. Controls were generally well matched except for more frequent comorbidities than the intervention groups and a different distribution of types of conditioning regimens used. Compared with controls, the hazard ratio for GRFS was 0·72 (90% CI 0·54-0·94; p=0·044) for tacrolimus, mycophenolate mofetil, and post-transplantation cyclophosphamide, 0·98 (0·76-1·27; p=0·92) for tacrolimus, methotrexate, and bortezomib, and 1·10 (0·86-1·41; p=0·49) for tacrolimus, methotrexate, and maraviroc. 238 patients experienced grade 3 or 4 toxicities: 12 (13%) had grade 3 and 67 (73%) grade 4 events with tacrolimus, mycophenolate mofetil, and post-transplantation cyclophosphamide; ten (11%) had grade 3 and 68 (76%) had grade 4 events with tacrolimus, methotrexate, and bortezomib; and 18 (20%) had grade 3 and 63 (68%) had grade 4 events with tacrolimus, methotrexate, and maraviroc. The most common toxicities were haematological (77 [84%] for tacrolimus, mycophenolate mofetil, and post-transplantation cyclophosphamide; 73 [82%] for tacrolimus, methotrexate, and bortezomib; and 78 [85%] for tacrolimus, methotrexate, and maraviroc) and cardiac (43 [47%], 44 [49%], and 43 [47%], respectively).
Interpretation: Tacrolimus, mycophenolate mofetil, and post-transplantation cyclophosphamide was the most promising intervention, yielding the best GRFS; this regimen is thus being prospectively compared with tacrolimus and methotrexate in a phase 3 randomised trial.
Funding: US National Health, Lung, and Blood Institute; National Cancer Institute; National Institute of Allergy and Infectious Disease; and Millennium Pharmaceuticals.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflicts of interest:
Ms. Bickett reports grants from NHLBI, during the conduct of the study.
Dr. Bolaños-Meade reports DSMB fees from Incyte Corporation, outside the submitted work.
Dr. Chen reports personal fees from Takeda, personal fees from Magenta, personal fees from Incyte, personal fees from Regimmune, personal fees from Kiadis, outside the submitted work.
Dr. Giralt reports grants from Blood and Marrow Transplant Clinical Trials Network, during the conduct of the study; grants and personal fees from CELGENE, grants and personal fees from TAKEDA, personal fees from JAZZ, grants from MITENYI, grants and personal fees from AMGEN, personal fees from Novartis, personal fees from KITE, grants from CSL Behring, personal fees from Bristol Myers Squibb, grants and personal fees from SANOFI, outside the submitted work. Dr. Holtan reports consulting fees from Incyte, outside the submitted work.
Dr. Koreth reports grants and non-financial support from Prometheus Labs, non-financial support from BMS, non-financial support from Novartis, non-financial support from Miltenyi Biotec, grants and non-financial support from Millennium, personal fees from Amgen, personal fees from Equillium Biotech, from Fortress Biotech, outside the submitted work.
Dr. Noel reports spousal income from Novartis Pharmaceutical, outside the submitted work.
Dr. Pasquini reports personal fees from Pfizer, personal fees from Medigene, outside the submitted work.
Dr. Reshef reports personal fees from Kite, personal fees from Bristol Myers, personal fees from Incyte, personal fees from Pfizer, personal fees from Pharmacyclics, personal fees from Exelixis, personal fees from Takeda, personal fees from Jazz Pharmaceuticals, outside the submitted work. Dr. Weisdorf reports grants from Incyte, outside the submitted work.
The other authors declared no conflict of interests.
Figures

References
-
- Bolaños-Meade J, Vogelsang GB. Acute graft-versus-host disease. Clin Adv Hematol Oncol 2004;2(10):672–82. - PubMed
-
- Bolaños-Meade J, Vogelsang GB. Chronic graft-versus-host disease. Curr Pharm Des 2008;14(20):1974–86. - PubMed
-
- Storb R, Deeg HJ, Whitehead J, Appelbaum F, Beatty P, Bensinger W, et al. Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. New England Journal of Medicine 1986;314:729–35. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 HL069294/HL/NHLBI NIH HHS/United States
- UG1 HL069290/HL/NHLBI NIH HHS/United States
- UG1 HL069249/HL/NHLBI NIH HHS/United States
- UG1 HL069310/HL/NHLBI NIH HHS/United States
- UG1 HL069315/HL/NHLBI NIH HHS/United States
- UG1 HL108945/HL/NHLBI NIH HHS/United States
- U10 HL069291/HL/NHLBI NIH HHS/United States
- UG1 HL069291/HL/NHLBI NIH HHS/United States
- P01 CA049605/CA/NCI NIH HHS/United States
- U24 CA076518/CA/NCI NIH HHS/United States
- U24 HL138660/HL/NHLBI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- UG1 HL109137/HL/NHLBI NIH HHS/United States
