

Epidemiology of Readmissions After Sepsis Hospitalization in Children
- PMID: 30824488
- PMCID: PMC6434975
- DOI: 10.1542/hpeds.2018-0175
Epidemiology of Readmissions After Sepsis Hospitalization in Children
Abstract
Background and objectives: The decline in hospital mortality in children hospitalized with sepsis has increased the number of survivors. These survivors are at risk for adverse long-term outcomes, including readmission and recurrent or unresolved infections. We described the epidemiology of 90-day readmissions after sepsis hospitalization in children. We tested the hypothesis that a sepsis hospitalization increases odds of 90-day readmissions.
Methods: Retrospective cohort analysis of the Nationwide Readmissions Database. We included index unplanned admissions of non-neonatal pediatric patients and described the proportion of readmissions, including those involving infection or sepsis. We performed multivariable analysis to determine the odds of readmission after a sepsis and nonsepsis admission and compared costs of readmission after sepsis and nonsepsis admissions.
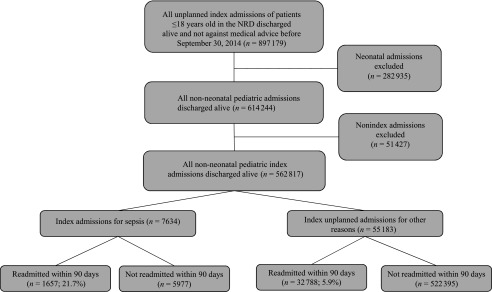
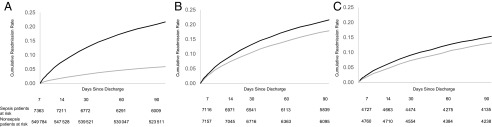
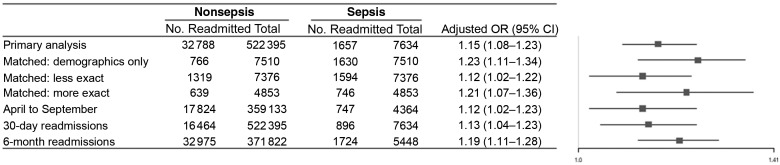
Results: Of 562 817 pediatric admissions, 7634 (1.4%) and 555 183 (98.6%) were discharged alive after admissions with and without sepsis. The rate of 90-day readmission after sepsis was 21.4%: 7.2% and 25.5% in previously healthy and chronically ill patients. The adjusted mean cost during readmission was $7385. Half of readmissions (52.9%) involved recurrent infection or sepsis. Sepsis admissions were associated with higher odds of readmission at 90 days compared with nonsepsis admissions (adjusted odds ratio 1.15, 95% confidence interval 1.08-1.23). The results remained unchanged for 30-day and 6-month readmissions.
Conclusions: Readmissions occur after 1 in 5 pediatric sepsis hospitalizations and increase health care costs. Sepsis hospitalization increased odds of readmission and commonly involved recurrent infection or sepsis. Clinicians caring for these patients should consider surveillance for recurrent or unresolved infection, and researchers should explore underlying mechanisms and potential interventions to reduce readmissions.
Copyright © 2019 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Readmission Diagnoses After Pediatric Severe Sepsis Hospitalization.Crit Care Med. 2019 Apr;47(4):583-590. doi: 10.1097/CCM.0000000000003646. Crit Care Med. 2019. PMID: 30676337 Free PMC article.
-
Post-Acute Care Use and Hospital Readmission after Sepsis.Ann Am Thorac Soc. 2015 Jun;12(6):904-13. doi: 10.1513/AnnalsATS.201411-504OC. Ann Am Thorac Soc. 2015. PMID: 25751120 Free PMC article.
-
Frequency, cost, and risk factors of readmissions among severe sepsis survivors.Crit Care Med. 2015 Apr;43(4):738-46. doi: 10.1097/CCM.0000000000000859. Crit Care Med. 2015. PMID: 25746745 Free PMC article.
-
Hospital readmission after surviving sepsis: A systematic review of readmission reasons and meta-analysis of readmission rates.J Crit Care. 2025 Feb;85:154925. doi: 10.1016/j.jcrc.2024.154925. Epub 2024 Oct 11. J Crit Care. 2025. PMID: 39393165
-
Reducing Readmission for Sepsis by Improving Risk Prediction Algorithms.Am J Crit Care. 2025 May 1;34(3):230-235. doi: 10.4037/ajcc2025455. Am J Crit Care. 2025. PMID: 40307178 Review.
Cited by
-
Children with severe sepsis: relationship between community level income and morbidity and mortality.Pediatr Res. 2023 Aug;94(2):837-844. doi: 10.1038/s41390-023-02500-w. Epub 2023 Feb 17. Pediatr Res. 2023. PMID: 36804502
-
Trajectory and Risk Factors of Persistent Decline in Health-Related Quality of Life after Septic Shock in Children with Preexisting Neurologic Disability.J Pediatr Intensive Care. 2022 Jan 18;13(3):242-252. doi: 10.1055/s-0041-1741402. eCollection 2024 Sep. J Pediatr Intensive Care. 2022. PMID: 39629157 Free PMC article.
-
Association of inflammatory biomarkers with new functional morbidity at hospital discharge in children who survive severe sepsis.Front Pediatr. 2025 Mar 7;13:1519246. doi: 10.3389/fped.2025.1519246. eCollection 2025. Front Pediatr. 2025. PMID: 40123667 Free PMC article.
-
Unplanned Admissions, Emergency Department Visits, and Epilepsy After Critical Neurological Illness Requiring Prolonged Mechanical Ventilation in Children.Neurohospitalist. 2023 Jan;13(1):31-39. doi: 10.1177/19418744221123628. Epub 2022 Oct 9. Neurohospitalist. 2023. PMID: 36531841 Free PMC article.
-
Utilizing big data from electronic health records in pediatric clinical care.Pediatr Res. 2023 Jan;93(2):382-389. doi: 10.1038/s41390-022-02343-x. Epub 2022 Nov 24. Pediatr Res. 2023. PMID: 36434202 Free PMC article. Review.
References
-
- Han YY, Carcillo JA, Dragotta MA, et al. Early reversal of pediatric-neonatal septic shock by community physicians is associated with improved outcome. Pediatrics. 2003;112(4):793–799 - PubMed
-
- Hartman ME, Linde-Zwirble WT, Angus DC, Watson RS. Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med. 2013;14(7):686–693 - PubMed
-
- Mayr FB, Talisa VB, Balakumar V, Chang CH, Fine M, Yende S. Proportion and cost of unplanned 30-day readmissions after sepsis compared with other medical conditions. JAMA. 2017;317(5):530–531 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
