

Intraarticular Glucocorticoid Injection as Second-line Treatment for Lyme Arthritis in Children
- PMID: 30824649
- PMCID: PMC6679761
- DOI: 10.3899/jrheum.180829
Intraarticular Glucocorticoid Injection as Second-line Treatment for Lyme Arthritis in Children
Abstract
Objective: To determine whether second-line intraarticular glucocorticoid (IAGC) injection improves outcomes in children with persistently active Lyme arthritis after initial antibiotics.
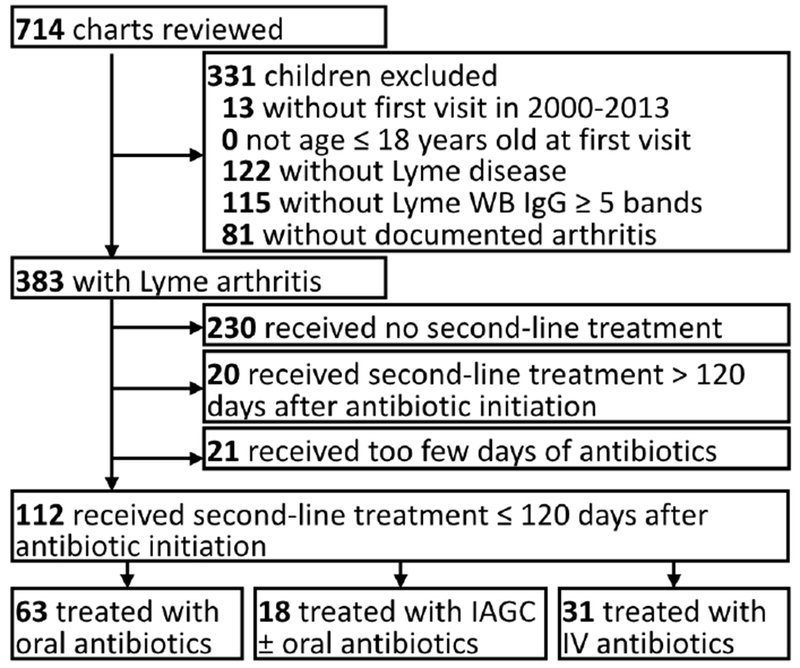
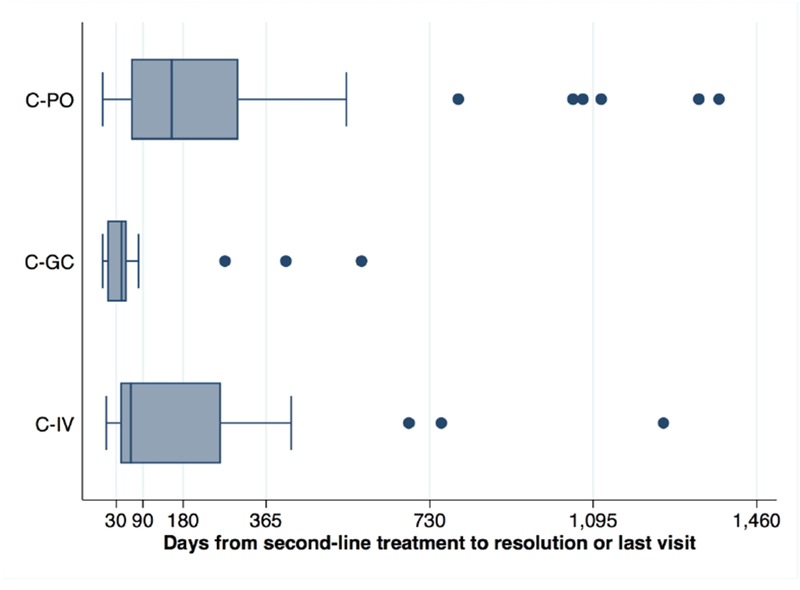
Methods: We conducted an observational comparative effectiveness study through chart review within 3 pediatric rheumatology centers with distinct clinical approaches to second-line treatment of Lyme arthritis. We primarily compared children receiving second-line IAGC to children receiving a second course of antibiotics alone. We evaluated the risk of developing antibiotic-refractory Lyme arthritis (ARLA) using logistic regression and the time to clinical resolution of Lyme arthritis using Cox regression.
Results: Of 112 children with persistently active Lyme arthritis after first-line antibiotics, 18 children received second-line IAGC (13 with concomitant oral antibiotics). Compared to children receiving second-line oral antibiotics alone, children treated with IAGC had similar baseline characteristics but lower rates of ARLA (17% vs 44%; OR 0.3, 95% CI 0.1-0.95; p = 0.04) and faster rates of clinical resolution (HR 2.2, 95% CI 1.2-3.9; p = 0.01). Children in IAGC and oral antibiotic cohorts did not differ in treatment-associated adverse events. Among children receiving second-line IAGC, outcomes appeared similar irrespective of use of concomitant antibiotics. Outcomes were also similar between intravenous (IV) and oral antibiotic-treated cohorts, but older children seemed to respond more favorably to IV therapy. IV antibiotics were also associated with higher rates of toxicity.
Conclusion: IAGC injection appears to be an effective and safe second-line strategy for persistent Lyme arthritis in children, associated with rapid clinical resolution and reduced need for additional treatment.
Keywords: COMPARATIVE EFFECTIVENESS RESEARCH; EPIDEMIOLOGIC STUDIES; GLUCOCORTICOIDS; LYME ARTHRITIS; PEDIATRICS.
Conflict of interest statement
Figures

Comment in
-
Treatment of Lyme Arthritis.J Rheumatol. 2019 Aug;46(8):871-873. doi: 10.3899/jrheum.190320. J Rheumatol. 2019. PMID: 31371661 No abstract available.
References
-
- Hubalek Z Epidemiology of Lyme borreliosis. Curr Probl Dermatol 2009;37:31–50. - PubMed
-
- Steere AC, Schoen RT, Taylor E. The clinical evolution of Lyme arthritis. Ann Intern Med 1987;107:725–31. - PubMed
-
- Gerber MA, Zemel LS, Shapiro ED. Lyme arthritis in children: clinical epidemiology and long-term outcomes. Pediatrics 1998;102:905–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical