

Cabozantinib in advanced non-clear-cell renal cell carcinoma: a multicentre, retrospective, cohort study
- PMID: 30827746
- PMCID: PMC6849381
- DOI: 10.1016/S1470-2045(18)30907-0
Cabozantinib in advanced non-clear-cell renal cell carcinoma: a multicentre, retrospective, cohort study
Abstract
Background: Cabozantinib is approved for patients with metastatic renal cell carcinoma on the basis of studies done in clear-cell histology. The activity of cabozantinib in patients with non-clear-cell renal cell carcinoma is poorly characterised. We sought to analyse the antitumour activity and toxicity of cabozantinib in advanced non-clear-cell renal cell carcinoma.
Methods: We did a multicentre, international, retrospective cohort study of patients with metastatic non-clear-cell renal cell carcinoma treated with oral cabozantinib during any treatment line at 22 centres: 21 in the USA and one in Belgium. Eligibility required patients with histologically confirmed non-clear-cell renal cell carcinoma who received cabozantinib for metastatic disease during any treatment line roughly between 2015 and 2018. Mixed tumours with a clear-cell histology component were excluded. No other restrictive inclusion criteria were applied. Data were obtained from retrospective chart review by investigators at each institution. Demographic, surgical, pathological, and systemic therapy data were captured with uniform database templates to ensure consistent data collection. The main objectives were to estimate the proportion of patients who achieved an objective response, time to treatment failure, and overall survival after treatment.
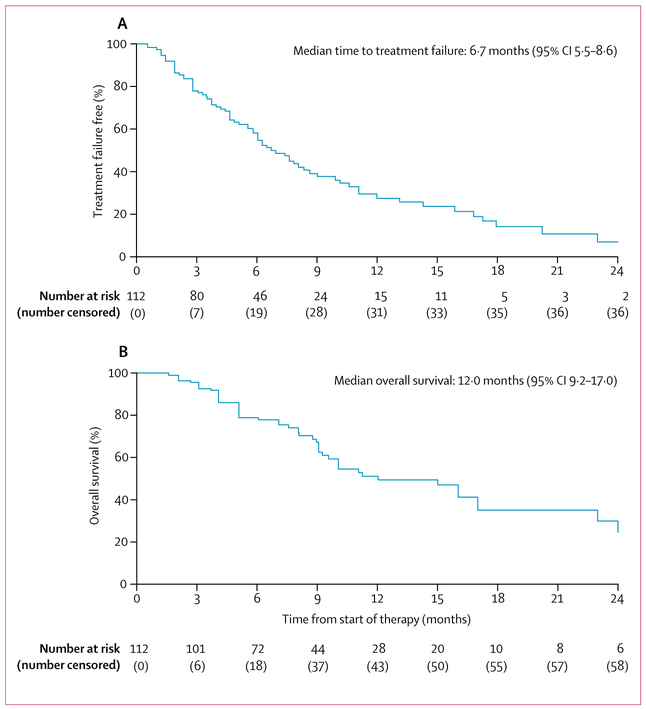
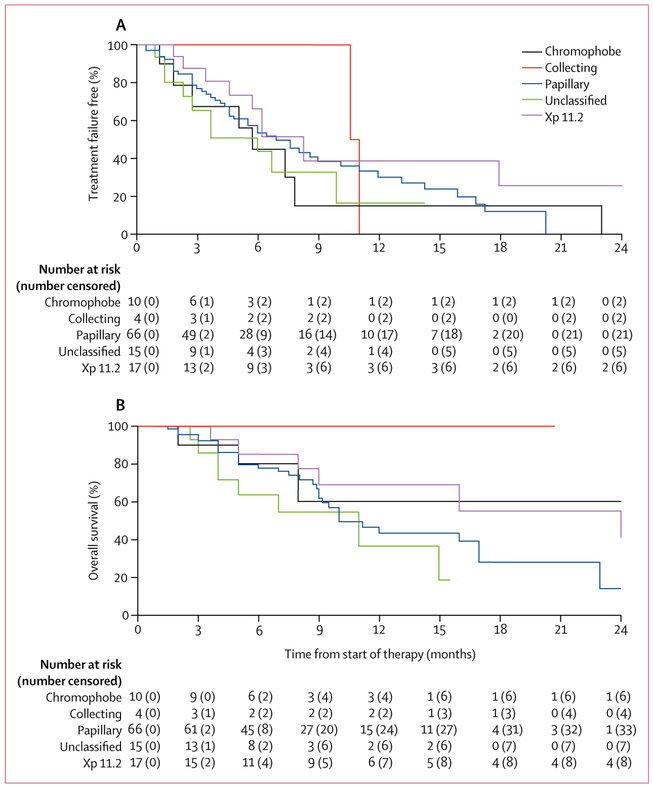
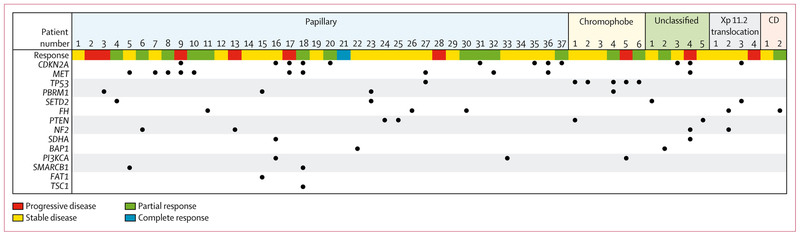
Findings: Of 112 identified patients with non-clear-cell renal cell carcinoma treated at the participating centres, 66 (59%) had papillary histology, 17 (15%) had Xp11.2 translocation histology, 15 (13%) had unclassified histology, ten (9%) had chromophobe histology, and four (4%) had collecting duct histology. The proportion of patients who achieved an objective response across all histologies was 30 (27%, 95% CI 19-36) of 112 patients. At a median follow-up of 11 months (IQR 6-18), median time to treatment failure was 6·7 months (95% CI 5·5-8·6), median progression-free survival was 7·0 months (5·7-9·0), and median overall survival was 12·0 months (9·2-17·0). The most common adverse events of any grade were fatigue (58 [52%]), and diarrhoea (38 [34%]). The most common grade 3 events were skin toxicity (rash and palmar-plantar erythrodysesthesia; five [4%]) and hypertension (four [4%]). No treatment-related deaths were observed. Across 54 patients with available next-generation sequencing data, the most frequently altered somatic genes were CDKN2A (12 [22%]) and MET (11 [20%]) with responses seen irrespective of mutational status.
Interpretation: While we await results from prospective studies, this real-world study provides evidence supporting the antitumour activity and safety of cabozantinib across non-clear-cell renal cell carcinomas. Continued support of international collaborations and prospective ongoing studies targeting non-clear-cell renal cell carcinoma subtypes and specific molecular alterations are warranted to improve outcomes across these rare diseases with few evidence-based treatment options.
Funding: None.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
NMC reports personal fees from Bayer and Pfizer WX reports personal fees from Bayer. MAB reports research founding from BMS, Nektar, Sanofi, Incyte, AstraZeneca, Genentech, Bayer, Tricon, Pfizer, and Seattle Genetics; and personal fees for advisory boards from Exelixis and Nektar. DMG reports personal fees for advisory boards from Exelixis. WS reports grant funding from AstraZeneca, Bayer, Bristol-Myers Squibb, Esai, Genentech, Pfizer, AbbVie, Astellas, Boehringer Ingelheim, Calithera, Clovis, Exilixis, Janssen, Merck, Seattle Genetics, Tesaro, and XP4 Pharmaceuticals; and personal fees from AstraZeneca, Bayer, Bristol-Myers Squibb, Caremark/CVS, Esai, Genentech, Pfizer, and Sotio. YZ reports personal fees for advisory board from Amgen, Roche Diagnostics, Novartis, Johnson & Johnson, Eisai, Exelixis, Pfizer, and Castle Bioscience. VN reports personal fees from Exelixis.BB reports personal fees from Ipsen, Merck, Amgen, Pfizer; and grant funding from BMS. RRM reports grant funding from Bayer and Pfizer; and personal fees for advisory board from Exelixis, BMS, Novartis, Tempus, and Janssen. RP reports grant funding from Ferring; and personal fees from AstraZeneca, BMS, Dendreon, Exelixis, Genentech/Roche, Merck, Sanofi-Genzyme, Jounce, EMD Serono, and Argos Therapeutics; and non-financial support from BMS, Dendreon, and Genentech/Roche. ETL reports grant funding from Exelixis. TLR reports grant funding from National Institute of Health. NV reports personal fees from Boehringer lngelheim. MRH reports personal fees from Argos, AstraZeneca, Exelixis, Genentech, and Pfizer; and grant funding from Bristol-Myers Squibb, Exelixis, Genentech, Merck, and Pfizer. AM reports personal fees for advisory board from Genetech/Roche; and institutional support for clinical trials from Acerta Pharma, Genentech/Roche, Seattle Genetics, Mirati Therapeutics, Bristol-Myers Squibb, and Roche. ERP reports grant funding from AstraZeneca, Bristol-Myers Squibb, Merck, Peloton, and Pfizer; and consulting funding from BMS, Exelexis, Genentech, Merck, Clovis, and Pfizer. UV reports grant funding and personal fees from Exelixis. SG reports grant funding from Pfizer, Merck, Agensys, BMS, Novartis, Bayer, and Eisai; and personal fees from AstraZeneca, Bayer, BMS, Novartis, Pfizer, Genentech, Exelixis, Janssen, Corvus, and Sanofi/Genzyme. NH reports personal fees from Merck, Novartis, Armo Biosciences, Pfizer, and BMS; and clinical research funding from Merck, SFJ Pharmaceuticals, and BMS. NA reports personal fees from consultancy from Astellas, AstraZeneca, Argos, BMS, Bayer, Clovis, Eisai, Exelixis, EMD Serono, Ely Lilly, Genentech, Merck, Medivation, Novartis, Nektar, and Pfizer; and grant research funding from Active Biotech, AstraZeneca, Bavarian Nordic, BMS, Calithera, Celldex, Eisai, Exelixis, Genetech, GlaxoSmithKline, Immunomedics, Janssen, Medivation, Merck, NewLink Genetics, Novartis, Pfizer, Prometheus, Rexahn, Sanofi, Takeda, and Tracon. SKP reports personal fees for consultancy and research from Pfizer, Novartis, AVEO, Myriad Genetics, Genentech, Exelixis, BMS, Astellas, and Medivation. DYCH reports grant funding and personal fees from BMS, Pfizer, Novartis, Ipsen, Exilexis, and Eisai. DB reports personal fees from BMS, Pfizer, and AstraZeneca. TKC reports grant funding, personal fees, and non-financial support from Pfizer and Exelixis; grant funding and personal fees from AstraZeneca, Bayer, BMS, Cerulean, Esai, Foundation Medicine, Exelixis, Genentech, Roche, GlaxoSmithKline, Merck, Novartis, Peloton, Pfizer, Prometheus Labs, Corvus, and Ipsen; grant funding from Tracon, Calithera, and Takeda outside the submitted work; and personal fees from Alligent, Up-to-Date, National Comprehensive Cancer Network, Analysis Group, Michael J Hennessy Associates (Healthcare Communications Company and several brands such as OnClive and PER), L-path, Kidney Cancer Journal, Clinical Care Options, Platform Q, Navinata Healthcare, Harborside Press,
Figures
Comment in
-
A well organised effort to metastatic non-clear-cell renal cell carcinoma.Lancet Oncol. 2019 Apr;20(4):472-473. doi: 10.1016/S1470-2045(19)30036-1. Epub 2019 Feb 28. Lancet Oncol. 2019. PMID: 30827747 No abstract available.
-
Another one in the chamber: cabozantinib for patients with metastatic non clear cell renal cell carcinoma.Ann Transl Med. 2019 Jul;7(Suppl 3):S137. doi: 10.21037/atm.2019.06.06. Ann Transl Med. 2019. PMID: 31576344 Free PMC article. No abstract available.
-
Cabozantinib in advanced non-clear-cell renal cell carcinoma: is it the way clearer now?Ann Transl Med. 2019 Sep;7(Suppl 6):S229. doi: 10.21037/atm.2019.07.70. Ann Transl Med. 2019. PMID: 31656808 Free PMC article. No abstract available.
References
-
- Giles RH, Choueiri TK, Heng DY, et al. Recommendations for the management of rare kidney cancers. Eur Urol 2017; 72: 974–83. - PubMed
-
- Moch H, Cubilla AL, Humphrey PA, Reuter VE, Ulbright TM. The 2016 WHO classification of tumours of the urinary system and male genital organs—part A: renal, penile, and testicular tumours. Eur Urol 2016; 70: 93–105. - PubMed
-
- Fernández-Pello S, Hofmann F, Tahbaz R, et al. A systematic review and meta-analysis comparing the effectiveness and adverse effects of different systemic treatments for non-clear cell renal cell carcinoma. Eur Urol 2017; 71: 426–36. - PubMed
-
- Hudes G, Carducci M, Tomczak P, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med 2007; 356: 2271–81. - PubMed
-
- Dutcher JP, de Souza P, McDermott C, et al. Effect of temsirolimus versus interferon-alpha on outcome of patients with advanced renal cell carcinoma of different tumor histologies. Med Oncol 2009; 26: 202–09. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
