

Physician agreement on the diagnosis of sepsis in the intensive care unit: estimation of concordance and analysis of underlying factors in a multicenter cohort
- PMID: 30828456
- PMCID: PMC6383290
- DOI: 10.1186/s40560-019-0368-2
Physician agreement on the diagnosis of sepsis in the intensive care unit: estimation of concordance and analysis of underlying factors in a multicenter cohort
Abstract
Background: Differentiating sepsis from the systemic inflammatory response syndrome (SIRS) in critical care patients is challenging, especially before serious organ damage is evident, and with variable clinical presentations of patients and variable training and experience of attending physicians. Our objective was to describe and quantify physician agreement in diagnosing SIRS or sepsis in critical care patients as a function of available clinical information, infection site, and hospital setting.
Methods: We conducted a post hoc analysis of previously collected data from a prospective, observational trial (N = 249 subjects) in intensive care units at seven US hospitals, in which physicians at different stages of patient care were asked to make diagnostic calls of either SIRS, sepsis, or indeterminate, based on varying amounts of available clinical information (clinicaltrials.gov identifier: NCT02127502). The overall percent agreement and the free-marginal, inter-observer agreement statistic kappa (κ free) were used to quantify agreement between evaluators (attending physicians, site investigators, external expert panelists). Logistic regression and machine learning techniques were used to search for significant variables that could explain heterogeneity within the indeterminate and SIRS patient subgroups.
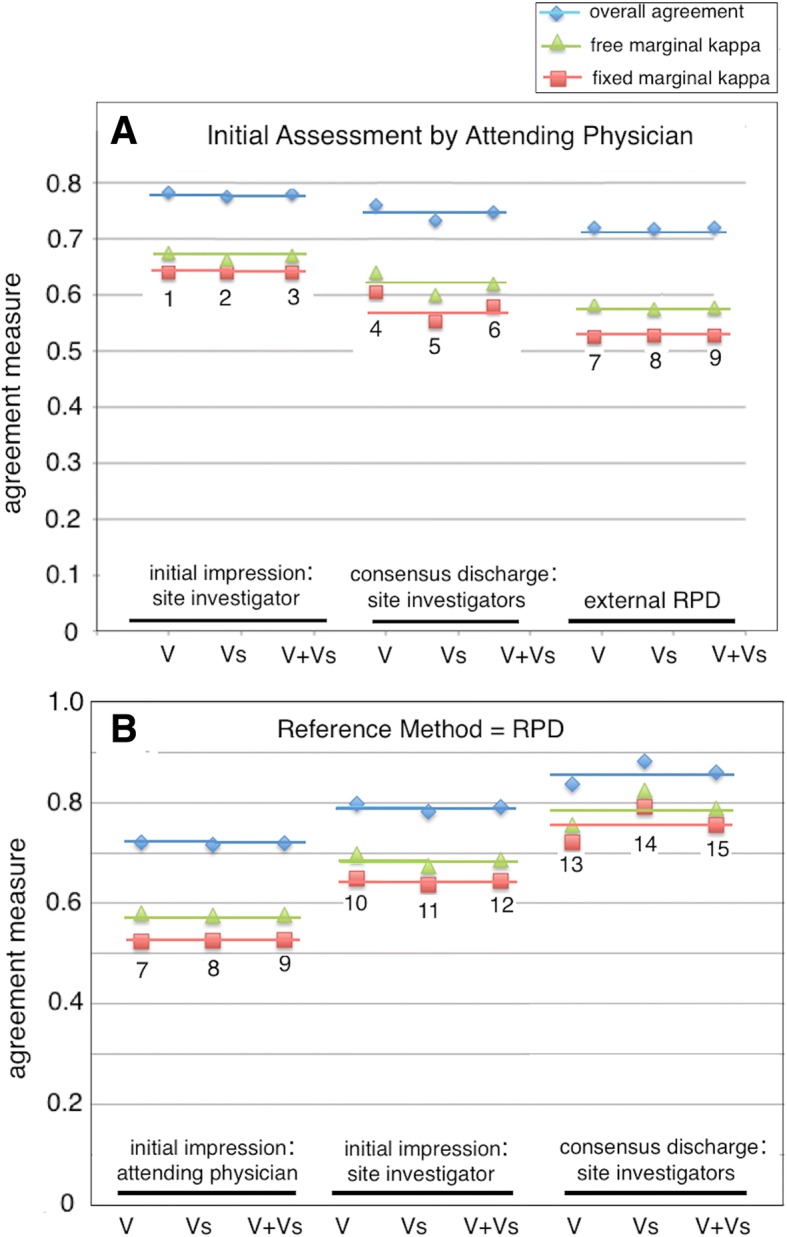
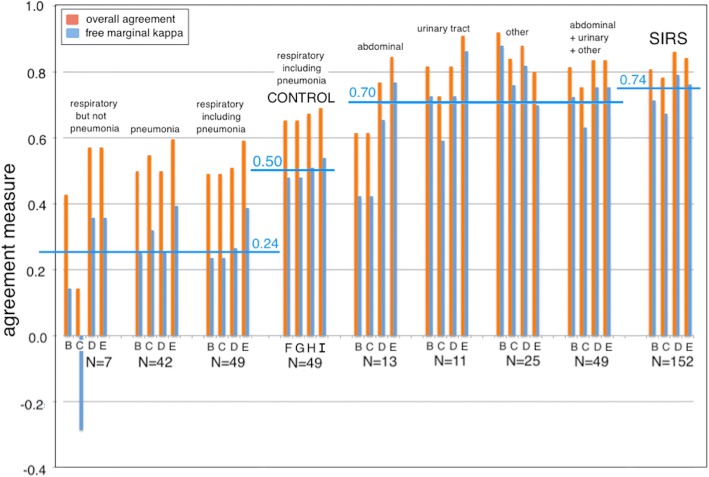
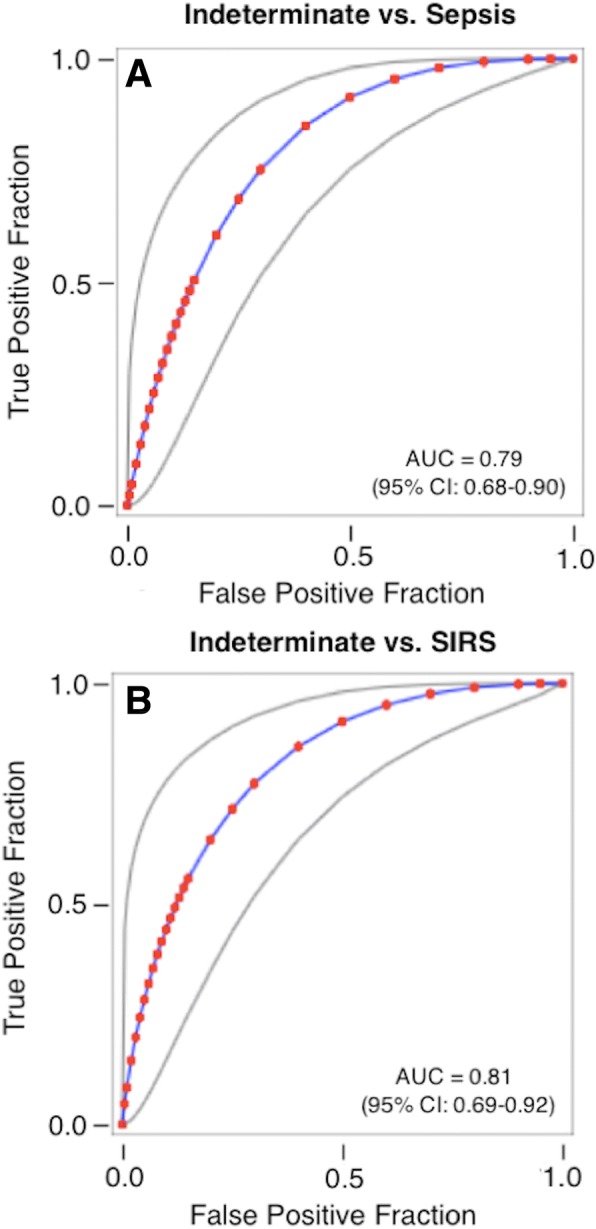
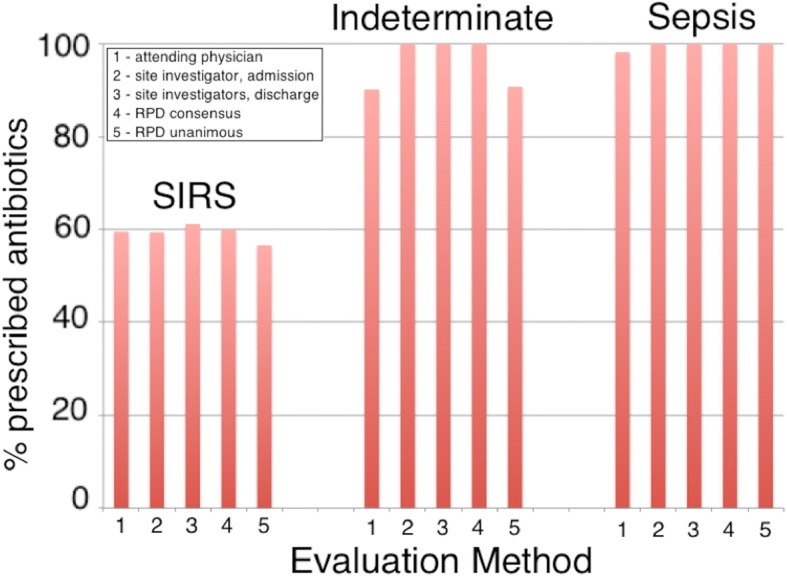
Results: Free-marginal kappa decreased between the initial impression of the attending physician and (1) the initial impression of the site investigator (κ free 0.68), (2) the consensus discharge diagnosis of the site investigators (κ free 0.62), and (3) the consensus diagnosis of the external expert panel (κ free 0.58). In contrast, agreement was greatest between the consensus discharge impression of site investigators and the consensus diagnosis of the external expert panel (κ free 0.79). When stratified by infection site, κ free for agreement between initial and later diagnoses had a mean value + 0.24 (range - 0.29 to + 0.39) for respiratory infections, compared to + 0.70 (range + 0.42 to + 0.88) for abdominal + urinary + other infections. Bioinformatics analysis failed to clearly resolve the indeterminate diagnoses and also failed to explain why 60% of SIRS patients were treated with antibiotics.
Conclusions: Considerable uncertainty surrounds the differential clinical diagnosis of sepsis vs. SIRS, especially before organ damage has become highly evident, and for patients presenting with respiratory clinical signs. Our findings underscore the need to provide physicians with accurate, timely diagnostic information in evaluating possible sepsis.
Keywords: Diagnosis; Intensive care; Inter-observer agreement; Sepsis.
Conflict of interest statement
Ethics approval was gained from the relevant institutional review boards: Intermountain Medical Center/Latter Day Saints Hospital (1024931); Johns Hopkins Hospital (IRB00087839); Rush University Medical Center (15111104-IRB01); Loyola University Medical Center (208291); Northwell Healthcare (16-02-42-03); and Grady Memorial Hospital (000-87806).This manuscript does not contain any individual person’s data in any form. Therefore, consent for publication is not required.The authors have read the journal’s policy and declare the following competing interests: LM, TDY, AR, RBB, RAB, and TS are current or past employees and/or shareholders of Immunexpress.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
