

Current Trends Among US Surgeons in the Identification, Treatment, and Time of Repair for Medial Meniscal Ramp Lesions at the Time of ACL Surgery
- PMID: 30828582
- PMCID: PMC6388449
- DOI: 10.1177/2325967119827267
Current Trends Among US Surgeons in the Identification, Treatment, and Time of Repair for Medial Meniscal Ramp Lesions at the Time of ACL Surgery
Abstract
Background: Given the potential hidden nature of medial meniscal ramp lesions and the controversy regarding treatment, it is important to understand the current trends regarding the identification and treatment strategies of meniscal ramp lesions by the leading surgeons and educators in the field of sports medicine.
Purpose: To better understand the current trends in orthopaedic surgery regarding arthroscopic identification and treatment of medial meniscal ramp lesions at the time of anterior cruciate ligament (ACL) surgery.
Study design: Cross-sectional study.
Methods: An electronic questionnaire was sent in a blinded fashion to 91 directors of orthopaedic sports medicine fellowship training programs in the United States. Participants' email addresses were obtained through the American Orthopaedic Society for Sports Medicine directory of current fellowship program directors. Inclusion criteria were only those surgeons who currently performed ACL reconstruction surgery. Exclusion criteria were those surgeons who did not perform ACL reconstruction or who chose to opt out of the survey.
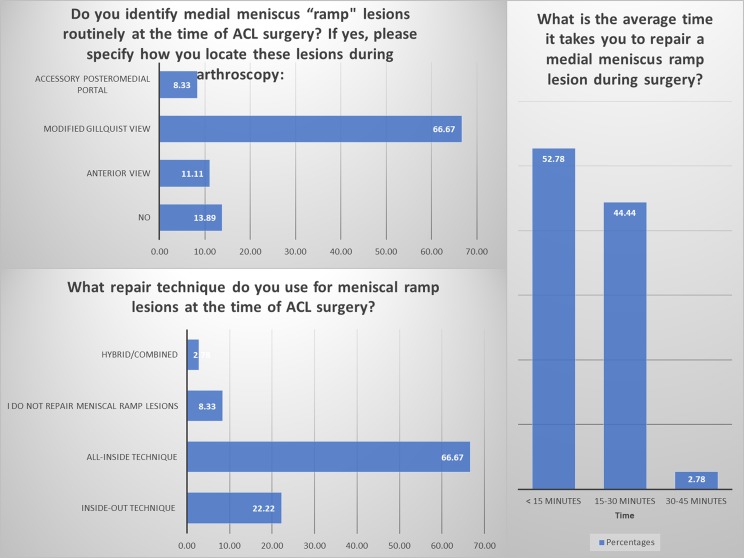
Results: Overall, 19 surgeons opted out of the survey; 36 responded from the remaining 72 surveys (50%). The majority (n = 31, 86%) reported routinely checking for a medial meniscal ramp lesion via inspection of the posteromedial meniscocapsular junction during an ACL reconstruction. The most common repair technique cited was all-inside (n = 24, 66.7%), followed by inside-out (n = 8, 22.2%). Three (8%) surgeons indicated that they did not repair meniscal ramp lesions. Regarding surgical treatment (repair vs no treatment), the majority reported using the extent of the tear (89%; partial vs full thickness) and the stability of the tear upon probing (81%) as the main criteria for intraoperative decision making. Nineteen (52.8%) surgeons required a mean time of <15 minutes for meniscal ramp repair; 16 surgeons (44.4%), 15 to 30 minutes; and 1 surgeon (2.8%), 30 to 45 minutes.
Conclusion: This study provides insight regarding meniscal ramp tear identification, treatment, and repair strategies from the fellowship directors of sports medicine orthopaedic surgery in the United States. Such information may be useful for current orthopaedic surgeons to advance their practice according to the current trends surrounding ACL reconstruction and medial meniscal ramp repair.
Keywords: anterior cruciate ligament reconstruction; medial meniscus; ramp lesion; survey.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest and source of funding: L.E. receives research support from Arthrex, Biomet, Smith & Nephew, and Health Southeast Norway and royalties from Arthrex and Smith & Nephew. R.F.L. receives educational support from Arthrex; is a consultant for Arthrex, Ossur, and Smith & Nephew; receives royalties from Arthrex, Ossur, and Smith & Nephew; is a paid speaker/presenter for Arthrex and Smith & Nephew; and has received hospitality payments from Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Arnoczky SP, Warren RF. Microvasculature of the human meniscus. Am J Sports Med. 1982;10(2):90–95. - PubMed
-
- Barber-Westin SD, Noyes FR. Clinical healing rates of meniscus repairs of tears in the central-third (red-white) zone. Arthroscopy. 2014;30(1):134–146. - PubMed
-
- DePhillipo NN, Cinque ME, Chahla J, Geeslin AG, Engebretsen L, LaPrade RF. Incidence and detection of meniscal ramp lesions on magnetic resonance imaging in patients with anterior cruciate ligament reconstruction. Am J Sports Med. 2017;45(10):2233–2237. - PubMed
-
- DePhillipo NN, Moatshe G, Brady A, et al. Effect of meniscocapsular and meniscotibial lesions in ACL-deficient and ACL-reconstructed knees: a biomechanical study. Am J Sports Med. 2018;46(10):2422–2431. - PubMed
LinkOut - more resources
Full Text Sources
