

Benign paroxysmal positional vertigo
- PMID: 30828628
- PMCID: PMC6383320
- DOI: 10.1002/lio2.230
Benign paroxysmal positional vertigo
Abstract
Objectives: Benign paroxysmal positional vertigo (BPPV) is the most common peripheral vestibular end-organ disease. This article aims to summarize research findings and key discoveries of BPPV. The pathophysiology, diagnosis, nonsurgical, and surgical management are discussed.
Methods: A comprehensive review of the literature regarding BPPV up through June 2018 was performed.
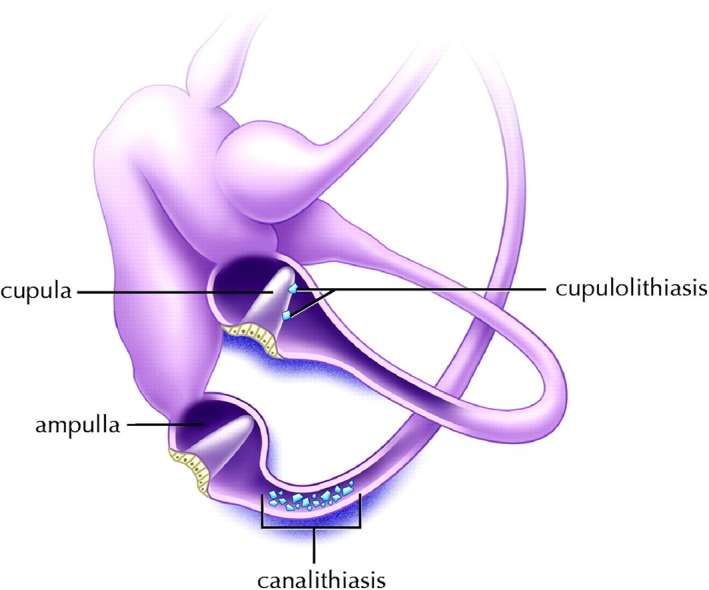
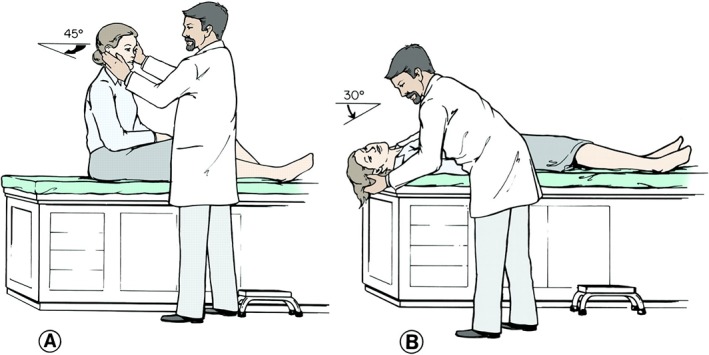
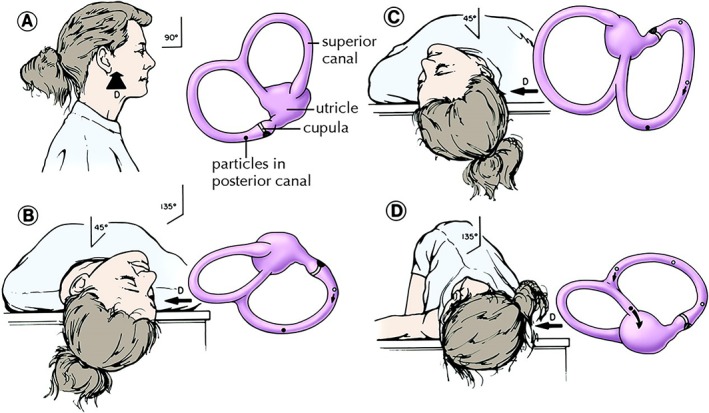
Results: BPPV is typified by sudden, brief episodes of vertigo precipitated by specific head movements. While often self-limited, BPPV can have a considerable impact on quality of life. The diagnosis can be established with a Dix-Hallpike maneuver for the posterior and anterior canals, or supine roll test for the horizontal canal, and typically does not require additional ancillary testing. Understanding the pathophysiology of both canalithiasis and cupulolithiasis has allowed for the development of various repositioning techniques. Of these, the particle repositioning maneuver is an effective way to treat posterior canal BPPV, the most common variant. Options for operative intervention are available for intractable cases or patients with severe and frequent recurrences.
Conclusions: A diagnosis of BPPV can be made through clinical history along with diagnostic maneuvers. BPPV is generally amenable to in-office repositioning techniques. For a small subset of patients with intractable BPPV, canal occlusion can be considered.
Level of evidence: N/A.
Keywords: Benign paroxysmal positional vertigo; Dix‐Hallpike; canalith; particle repositioning maneuver; semicircular canal occlusion.
Figures
References
-
- Katsarkas A. Benign paroxysmal positional vertigo (BPPV): idiopathic versus post‐traumatic. Acta Otolaryngol 1999;119(7):745–749. - PubMed
-
- Kim J‐S, Zee DS. Benign Paroxysmal Positional Vertigo. N Engl J Med 2014;370(12):1138–1147. - PubMed
-
- Mizukoshi K, Watanabe Y, Shojaku H, Okubo J, Watanabe I. Epidemiological studies on benign paroxysmal positional vertigo in Japan. Acta Otolaryngol Suppl 1988;447:67–72. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials