

Palatal anatomy for sleep apnea surgery
- PMID: 30828637
- PMCID: PMC6383450
- DOI: 10.1002/lio2.238
Palatal anatomy for sleep apnea surgery
Abstract
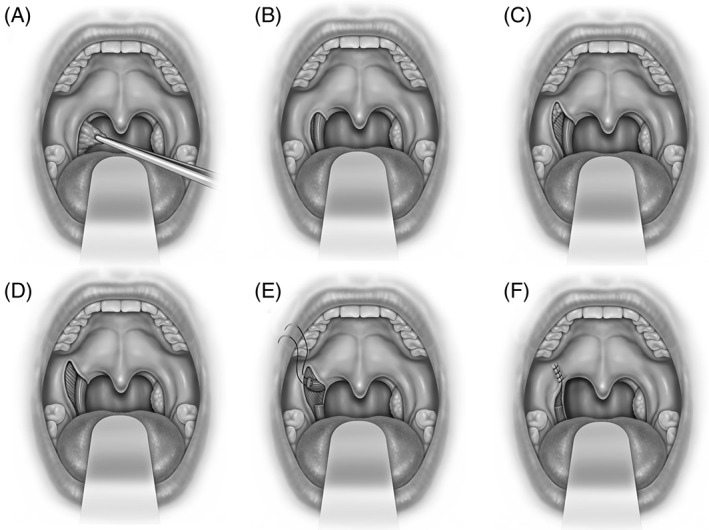
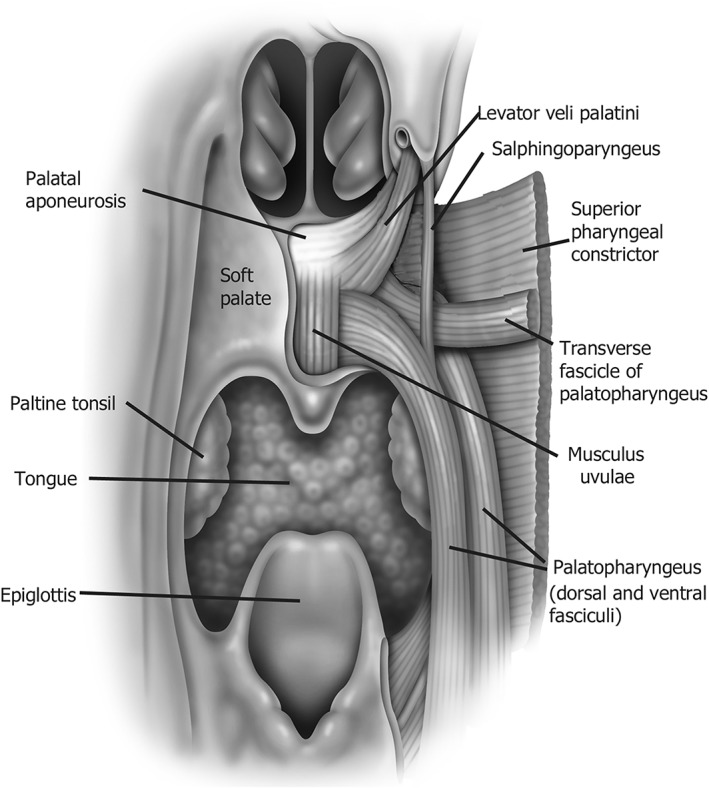
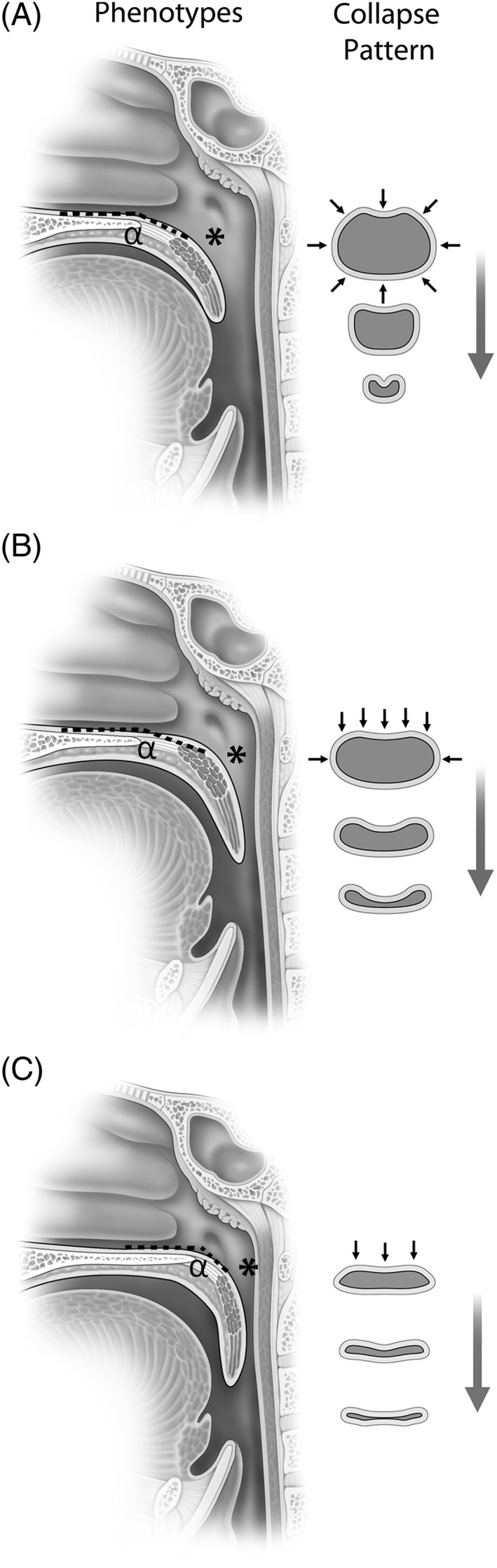
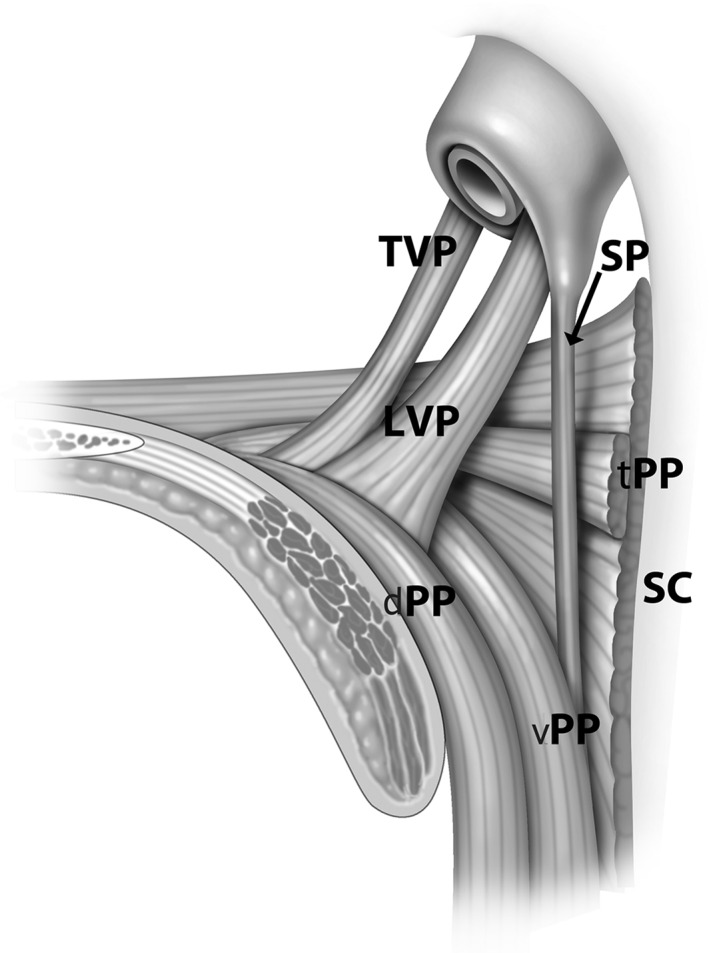
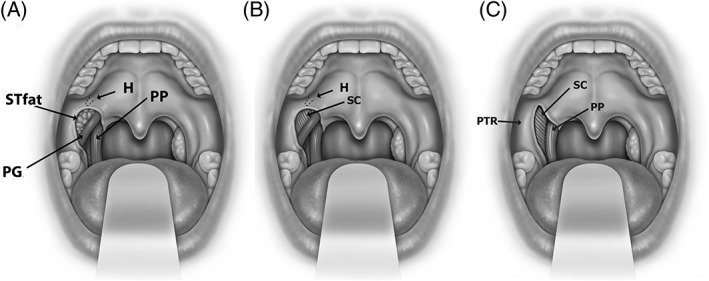
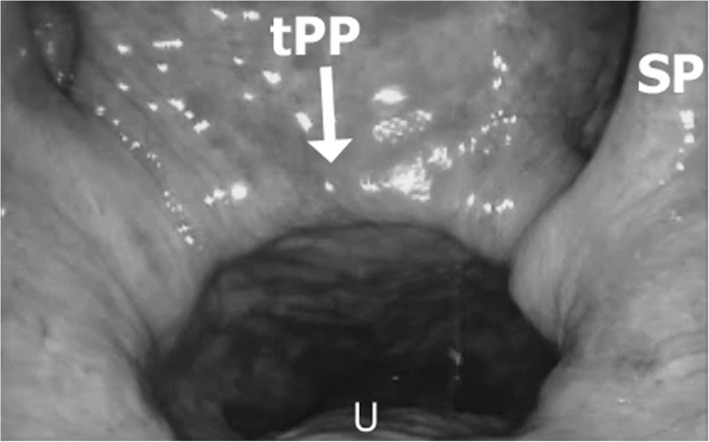
The goal of this review is to advance the understanding of the muscular and soft tissue palatal anatomy as it relates to palatal surgery for sleep apnea and the phenotypic variations that generate the shape and collapsibility of the retropalatal airway. Anatomically, the soft palate has both a proximal and distal segments separated by the palatal genu. The proximal palatal segment has a variable angle from the hard palate (ie, alpha angle) determined by the position and length of the levator veli palatini muscle. The palatopharyngeus muscle (PP) is a major defining element of the palate and lateral pharyngeal wall and forms the medial wall of the lateral palatal space. It is composed of two divisions: the longitudinal palatopharyngeus fasciculi which acts to elevate the pharynx and depress the soft palate and the transverse palatopharyngeus fascicle (Passavant's ridge) which function is a nasopharyngeal sphincter. The lateral palatal space incorporates the supra-tonsilar fat, and is bounded by muscles that determine the structure of the palate and associated lateral pharyngeal walls. Understanding of palatal muscles and pharyngeal airway phenotypes provides insight into the steps and mechanisms of pharyngoplasty procedures.
Level of evidence: N/A.
Keywords: Palatopharyngeus; anatomy; lateral palatal space; obstructive sleep apnea; palate; pharyngoplasty; phenotypes.
Figures
References
-
- Pang KP, Woodson BT. Expansion sphincter pharyngoplasty: a new technique for the treatment of obstructive sleep apnea. Otolaryngol Head Neck Surg 2007;137(1):110–114. - PubMed
-
- Cahali MB. Lateral pharyngoplasty: a new treatment for OSAHS. Laryngoscope 2003;113:1961–1968. - PubMed
-
- Han D, Ye J, Lin Z, Wang J, Wang J, Zhang Y. Revised uvulopalatopharyngoplasty with uvula preservation and its clinical study. ORL J Otorhinolaryngol Relat Spec 2005;67(4):213–219. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous