

Treatment-induced brain tissue necrosis: a clinical challenge in neuro-oncology
- PMID: 30828724
- PMCID: PMC7594558
- DOI: 10.1093/neuonc/noz048
Treatment-induced brain tissue necrosis: a clinical challenge in neuro-oncology
Abstract
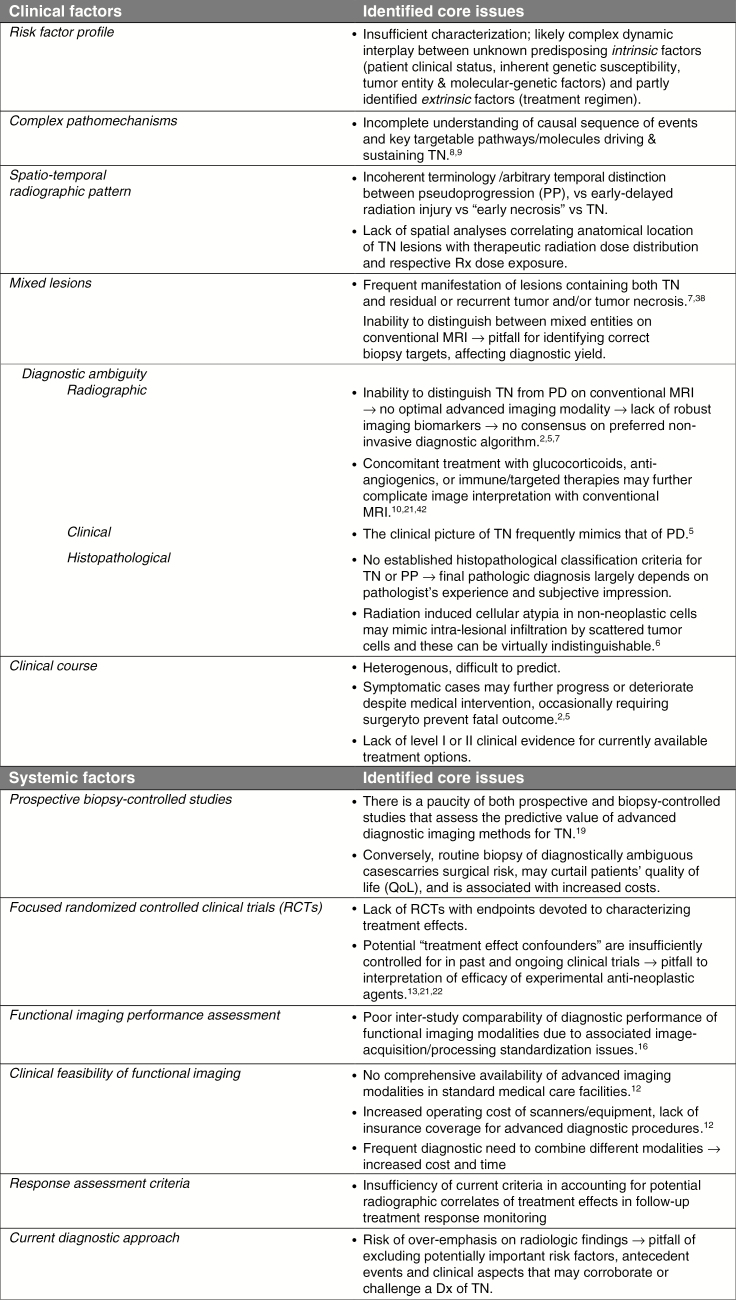
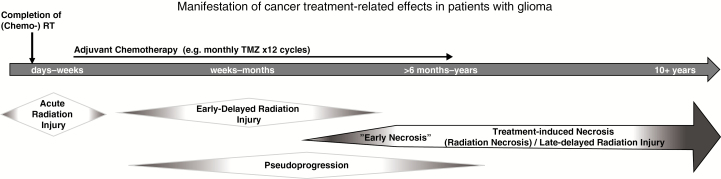
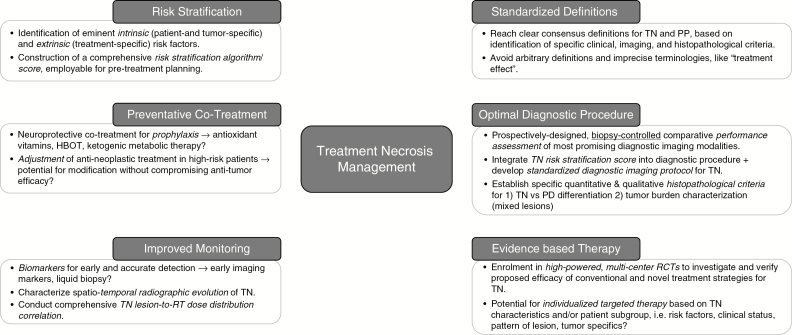
Cancer therapy-induced adverse effects on the brain are a major challenge in neuro-oncology. Brain tissue necrosis (treatment necrosis [TN]) as a consequence of brain directed cancer therapy remains an insufficiently characterized condition with diagnostic and therapeutic difficulties and is frequently associated with significant patient morbidity. A better understanding of the underlying mechanisms, improvement of diagnostic tools, development of preventive strategies, and implementation of evidence-based therapeutic practices are pivotal to improve patient management. In this comprehensive review, we address existing challenges associated with current TN-related clinical and research practices and highlight unanswered questions and areas in need of further research with the ultimate goal to improve management of patients affected by this important neuro-oncological condition.
Keywords: complications; malignant glioma; radiation necrosis; treatment effects; treatment necrosis.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

References
-
- Dietrich J, Winter SF, Klein JP. Neuroimaging of brain tumors: pseudoprogression, pseudoresponse, and delayed effects of chemotherapy and radiation. Semin Neurol. 2017;37(5):589–596. - PubMed
-
- Dietrich J, Klein JP. Imaging of cancer therapy-induced central nervous system toxicity. Neurol Clin. 2014;32(1):147–157. - PubMed
-
- Giglio P, Gilbert MR. Cerebral radiation necrosis. Neurologist. 2003;9(4):180–188. - PubMed
-
- Na A, Haghigi N, Drummond KJ. Cerebral radiation necrosis. Asia Pac J Clin Oncol. 2014;10(1):11–21. - PubMed
-
- Eisele SC, Dietrich J. Cerebral radiation necrosis: diagnostic challenge and clinical management. Rev Neurol. 2015;61(5):225–232. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
