

Clinical characteristics of hospitalized heart failure patients with preserved, mid-range, and reduced ejection fractions in Japan
- PMID: 30829002
- PMCID: PMC6487690
- DOI: 10.1002/ehf2.12418
Clinical characteristics of hospitalized heart failure patients with preserved, mid-range, and reduced ejection fractions in Japan
Abstract
Aims: There are regional differences in the patient characteristics, management, and outcomes of hospitalized patients with heart failure (HF). The aim of this study was to evaluate the clinical characteristics and outcomes of Japanese patients who are hospitalized with HF on the basis of the left ventricular ejection fraction (LVEF) stratum.
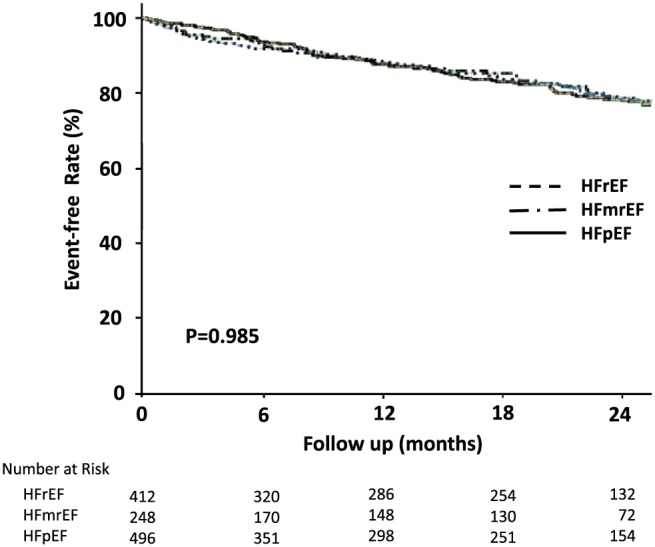
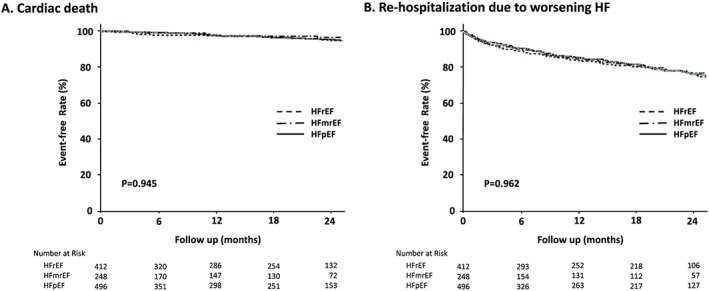
Methods and results: We retrospectively conducted a multicentre cohort study of 1245 hospitalized patients with decompensated HF between 2013 and 2014. Of these patients, 36% had an LVEF < 40% [HF with reduced ejection fraction (HFrEF), median age 72 years, 71% male], 21% had an LVEF 40-49% [HF with mid-range EF (HFmrEF), 77 years, 56% male], and 43% had an LVEF ≥ 50% [HF with preserved EF (HFpEF), 81 years, 44% male]. The primary outcome was death from any cause, and the secondary outcomes were cardiac death and re-hospitalization due to worsened HF after hospital discharge. There were high proportions of non-ischaemic cardiomyopathy (32%) in HFrEF patients, coronary artery disease (44%) in HFmrEF patients, and valvular disease (39%) in HFpEF patients. The frequencies of intravenous diuretic and natriuretic peptide administration during hospitalization were 66% and 30%, respectively. The median hospital stay for the overall population was 19 days, and the length of stay was >7 days for >90% of patients. In-hospital mortality was 7%, but was not different among the LVEF groups (HFrEF 7%, HFmrEF 6%, and HFpEF 8%). After a median follow-up of 19 months (range, 3-26 months), 192 (17%) of the 1156 patients who were discharged alive died, and 534 (46%) were re-hospitalized after hospital discharge. There were no significant differences in mortality after hospital discharge among the three LVEF groups (HFrEF 18%, HFmrEF 16%, and HFpEF 16%). There were no differences in cardiac death or re-hospitalization due to worsened HF after hospital discharge among the LVEF groups (cardiac death: HFrEF 8%, HFmrEF 7%, and HFpEF 7%; re-hospitalization due to worsened HF: HFrEF 19%, HFmrEF 16%, and HFpEF 17%). Multivariable-adjusted analyses showed that the HFmrEF and HFrEF groups, compared with the HFpEF group, were not associated with an increased risk for in-hospital death or death after hospital discharge. Non-cardiac causes of death and re-hospitalization after hospital discharge accounted for 35% and 38%, respectively.
Conclusions: Our results revealed different clinical characteristics but similar mortality rates in the HFrEF, HFmrEF, and HFpEF groups. The most common cause of death and re-hospitalization after hospital discharge was HF, but non-cardiac causes also contributed to their prognosis. Integrated management approaches will be required for HF patients.
Keywords: Heart failure; Hospitalization; Japanese; Left ventricular ejection fraction; Mortality.
© 2019 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
Dr Shiga received lecture fees from Eisai, Toa Eiyo, Bayer, and Daiichi‐Sankyo. Dr Hagiwara received research funding from Eisai, Nippon Boehringer Ingelheim, and Daiichi‐Sankyo and received lecture fees from Nippon Boehringer Ingelheim and Bristol‐Myers Squibb. The other authors have nothing to disclose.
Figures
References
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, Nodari S, Lam CSP, Sato N, Shah AN, Gheorghiade M. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol 2014; 63: 1123–1133. - PubMed
-
- Sakata Y, Shimokawa H. Epidemiology of heart failure in Asia. Circ J 2013; 77: 2209–2217. - PubMed
-
- Okamoto H, Kitabatake A. The epidemiology of heart failure in Japan. Nihon Rinsho 2003; 61: 709–714 (in Japanese). - PubMed
-
- Okura Y, Ramadan MM, Ohno Y, Mitsuma W, Tanaka K, Ito M, Suzuki K, Tanabe N, Kodama M, Aizawa Y. Impending epidemic: future projection of heart failure in Japan to the year 2055. Circ J 2008; 72: 489–491. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous