

Culture-Negative and Culture-Positive Sepsis: A Comparison of Characteristics and Outcomes
- PMID: 30829670
- PMCID: PMC7577261
- DOI: 10.1213/ANE.0000000000004072
Culture-Negative and Culture-Positive Sepsis: A Comparison of Characteristics and Outcomes
Abstract
Background: The primary objective of this study was to compare the characteristics of culture-positive and culture-negative status in septic patients. We also determined whether culture status is associated with mortality and whether unique variables are associated with mortality in culture-positive and culture-negative patients separately.
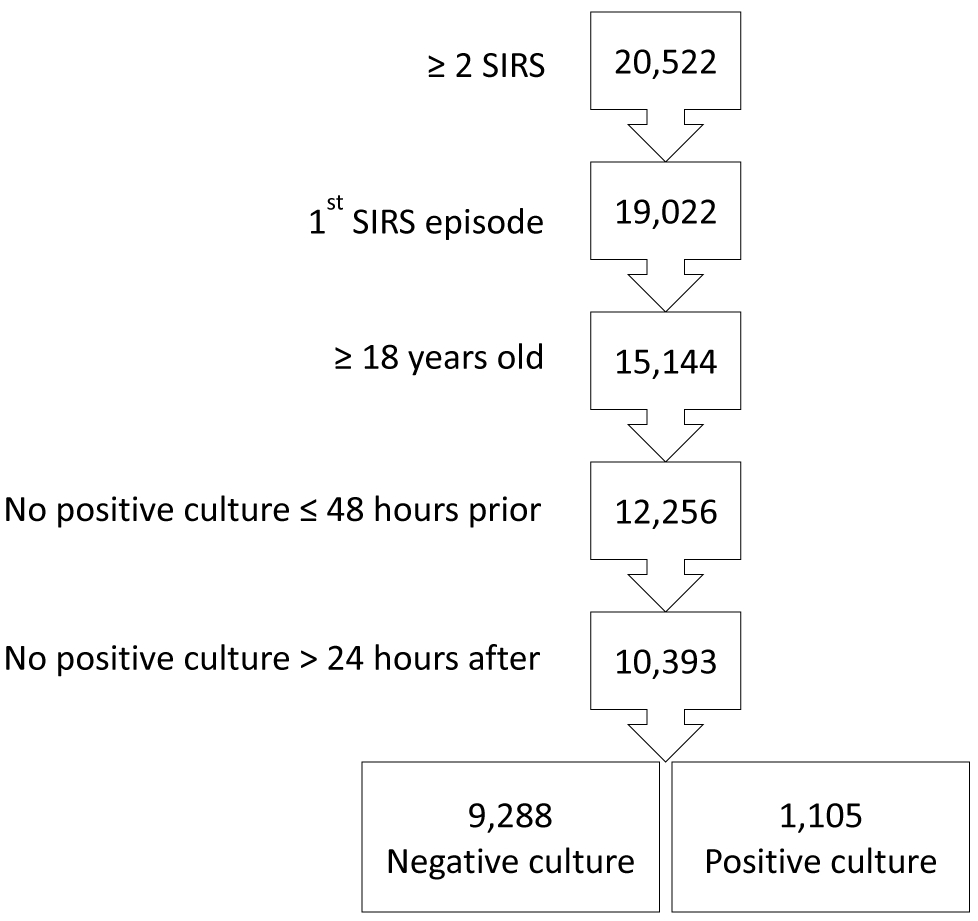
Methods: Utilizing patient records from intensive care units, emergency department, and general care wards in a large academic medical center, we identified adult patients with suspected infection and ≥2 systemic inflammatory response syndrome criteria between January 1, 2007, and May 31, 2014. We compared the characteristics between culture-positive and culture-negative patients and used binary logistic regression to identify variables independently associated with culture status and mortality. We also did sensitivity analyses using patients with Sequential Organ Failure Assessment and quick Sequential Organ Failure Assessment criteria for sepsis.
Results: The study population included 9288 culture-negative patients (89%) and 1105 culture-positive patients (11%). Culture-negative patients received more antibiotics during the 48 hours preceding diagnosis but otherwise demonstrated similar characteristics as culture-positive patients. After adjusting for illness severity, a positive culture was not independently associated with mortality (odds ratio = 1.01 [95% CI, 0.81-1.26]; P = .945). The models predicting mortality separately in culture-negative and culture-positive patients demonstrated very good and excellent discrimination (C-statistic ± SD, 0.87 ± 0.01 and 0.92 ± 0.01), respectively. In the sensitivity analyses using patients with sepsis by Sequential Organ Failure Assessment and quick Sequential Organ Failure Assessment criteria, after adjustments for illness severity, positive cultures were still not associated with mortality (odds ratio = 1.13 [95% CI, 0.86-1.43]; P = .303; and odds ratio = 1.05 [95% CI, 0.83-1.33]; P = .665), respectively. In all models, physiological derangements were associated with mortality.
Conclusions: While culture status is important for tailoring antibiotics, culture-negative and culture-positive patients with sepsis demonstrate similar characteristics and, after adjusting for severity of illness, similar mortality. The most important factor associated with negative cultures is receipt of antibiotics during the preceding 48 hours. The risk of death in patients suspected of having an infection is most associated with severity of illness. This is aligned with the Sepsis-3 definition using Sequential Organ Failure Assessment score to better identify those suspected of infection at highest risk of a poor outcome.
Conflict of interest statement
The above authors have no conflicts of interest and no financial disclosures.
Figures
References
-
- Kumar G, Kumar N, Taneja A, Kaleekal T, Tarima S, McGinley E et al.: Nationwide trends of severe sepsis in the 21st century (2000-2007). Chest. 2011;140:1223–31. - PubMed
-
- Bone RC, Balk RA, Cerra FB: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644–1655. - PubMed
-
- Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med. 2015;372:1629–38. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
