

Comparison of the efficacy of erector spinae plane block performed with different concentrations of bupivacaine on postoperative analgesia after mastectomy surgery: ramdomized, prospective, double blinded trial
- PMID: 30832580
- PMCID: PMC6399855
- DOI: 10.1186/s12871-019-0700-3
Comparison of the efficacy of erector spinae plane block performed with different concentrations of bupivacaine on postoperative analgesia after mastectomy surgery: ramdomized, prospective, double blinded trial
Abstract
Background: Breast cancer surgery is one of the most common surgeries among the female population. Nearly half of the patients suffer chronic pain following breast cancer surgery, and 24% of them categorizing their pain as moderate to high. In this study, effects of ultrasound-guided erector spinae plane (ESP) block performed using two different concentrations of bupivacaine on postoperative tramadol consumption, pain scores, and intraoperative fentanyl requirements among patients who underwent radical mastectomy surgery were compared.
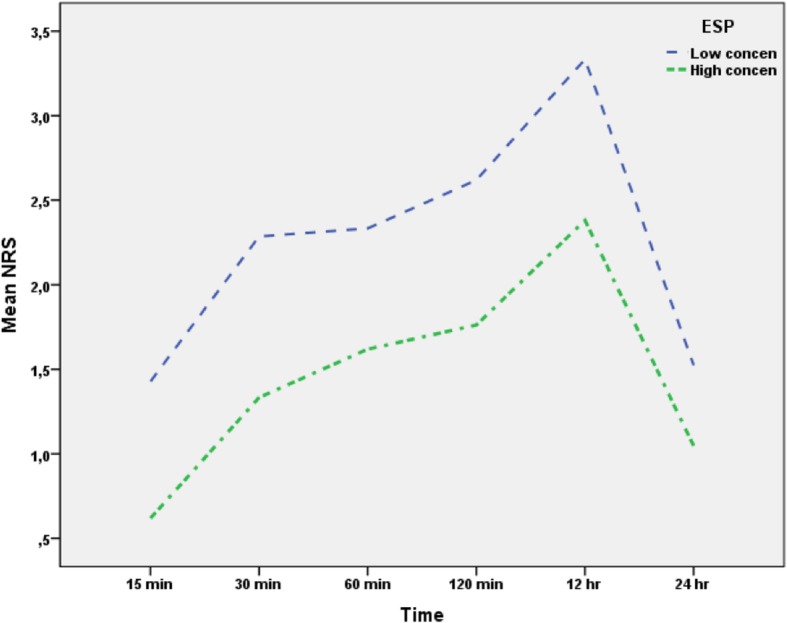
Methods: This double-blinded, prospective, and randomized study included patients with age ranged 18-70, American Society of Anesthesiologist physical status I-II, and scheduled for unilateral modified radical mastectomy surgery. The patients were randomly allocated into two groups. In group I, ESP block was performed with 0.375% bupivacaine. In group II, ESP block was performed with 0.25% bupivacaine. General anesthesia was induced in both groups according to the standard procedures. When the pain score was ≥4, patients received intravenous (i.v.) 25 mcg fentanyl in the recovery room or 4 mg of morphine in the surgical ward as a rescue analgesia. The main measurements were postoperative tramadol consumption; Numerical Rating Scale (NRS) scores 15, 30, and 60 min and 12 and 24 h postoperatively; and intraoperative fentanyl requirements.
Results: In total, 42 patients (21 patients in each group) were included in the study. The mean tramadol consumption at the postoperative 24th h was 149.52 ± 25.39 mg in group I, and 199.52 ± 32.78 mg in group II (p = 0.001). In group I, the NRS scores were significantly lower at every time points compared with those in group II. The mean intraoperative fentanyl requirement was similar in the two groups.
Conclusion: Although ESP block performed with both concentrations of bupivacaine provided effective postoperative analgesia, the higher concentration of bupivacaine significantly reduced postoperative tramadol consumption after radical mastectomy surgery.
Clinical trial registration: The study was registered prospectively with the Australian New Zealand Clinical Trials Registry (trial ID: ACTRN12618001334291at 08/08/2018).
Keywords: Analgesia; Erector spinae plane block; Mastectomy; Postoperative pain; Ultrasound.
Conflict of interest statement
Ethics approval and consent to participate
This study has been approved by Muğla Sıtkı Koçman University Clinical Research Ethics Committee with decision number: 02–07. A written informed consent form was obtained from all patients agreed to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
