

Postoperative remote lung injury and its impact on surgical outcome
- PMID: 30832647
- PMCID: PMC6399848
- DOI: 10.1186/s12871-019-0698-6
Postoperative remote lung injury and its impact on surgical outcome
Abstract
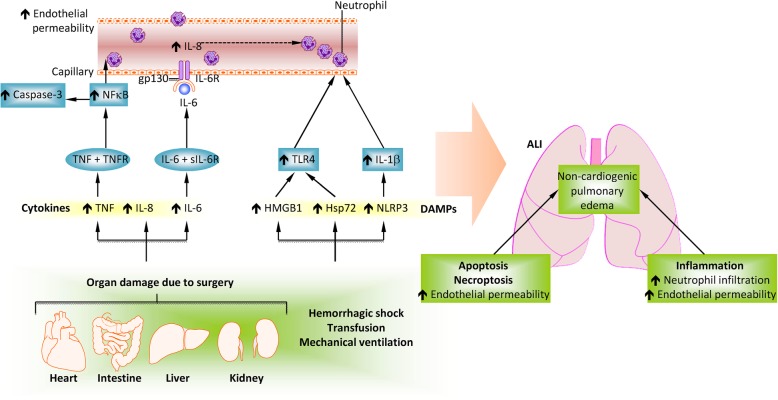
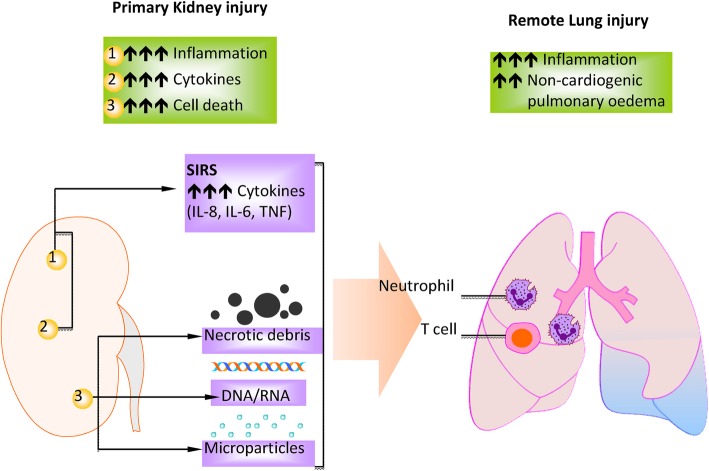
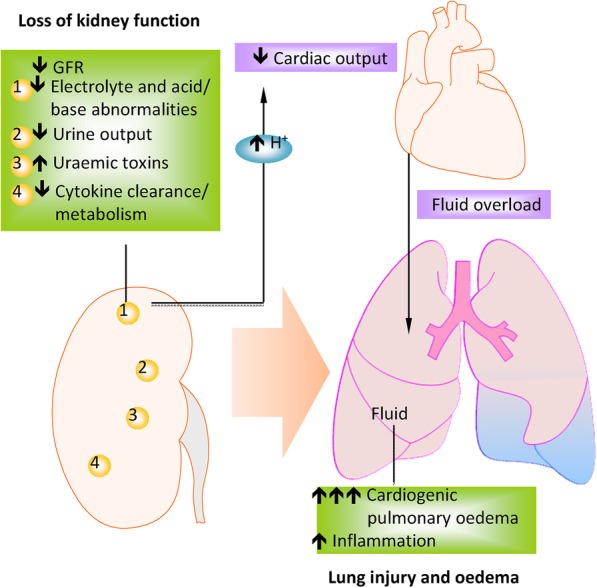
Postoperative remote lung injury is a complication following various surgeries and is associated with short and long-term mortality and morbidity. The release of proinflammatory cytokines, damage-associated molecular patterns such as high-mobility group box-1, nucleotide-biding oligomerization domain (NOD)-like receptor protein 3 and heat shock protein, and cell death signalling activation, trigger a systemic inflammatory response, which ultimately results in organ injury including lung injury. Except high financial burden, the outcome of patients developing postoperative remote lung injury is often not optimistic. Several risk factors had been classified to predict the occurrence of postoperative remote lung injury, while lung protective ventilation and other strategies may confer protective effect against it. Understanding the pathophysiology of this process will facilitate the design of novel therapeutic strategies and promote better outcomes of surgical patients. This review discusses the cause and pathology underlying postoperative remote lung injury. Risk factors, surgical outcomes and potential preventative/treatment strategies against postoperative remote lung injury are also addressed.
Keywords: Cytokine; Pathophysiology; Remote lung injury; Risk factor; Therapeutic strategy.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Daqing Ma is an editorial board member for BMC Anesthesiology. The other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Canet J, Gallart L, Gomar C, Paluzie G, Valles J, Castillo J, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338–1350. - PubMed
-
- Fernandez-Perez ER, Sprung J, Afessa B, Warner DO, Vachon CM, Schroeder DR, et al. Intraoperative ventilator settings and acute lung injury after elective surgery: a nested case control study. Thorax. 2009;64(2):121–127. - PubMed
-
- Herridge MS, Tansey CM, Matte A, Tomlinson G, Diaz-Granados N, Cooper A, et al. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364(14):1293–1304. - PubMed
-
- Dimick JB, Chen SL, Taheri PA, Henderson WG, Khuri SF, Campbell DJ. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg. 2004;199(4):531–537. - PubMed
-
- Menis M, Anderson SA, Forshee RA, McKean S, Johnson C, Warnock R, et al. Transfusion-related acute lung injury and potential risk factors among the inpatient US elderly as recorded in Medicare claims data, during 2007 through 2011. Transfusion. 2014;54(9):2182–2193. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
