

The pathology of small airways disease in COPD: historical aspects and future directions
- PMID: 30832670
- PMCID: PMC6399904
- DOI: 10.1186/s12931-019-1017-y
The pathology of small airways disease in COPD: historical aspects and future directions
Abstract
Small airways disease (SAD) is a cardinal feature of chronic obstructive pulmonary disease (COPD) first recognized in the nineteenth century. The diverse histopathological features associated with SAD underpin the heterogeneous nature of COPD. Our understanding of the key molecular mechanisms which drive the pathological changes are not complete. In this article we will provide a historical overview of key histopathological studies which have helped shape our understanding of SAD and discuss the hallmark features of airway remodelling, mucous plugging and inflammation. We focus on the relationship between SAD and emphysema, SAD in the early stages of COPD, and the mechanisms which cause SAD progression, including bacterial colonization and exacerbations. We discuss the need to specifically target SAD to attenuate the progression of COPD.
Keywords: Bacteria; COPD; Emphysema; Exacerbations; Histopathology; Inflammation; Remodeling; Small airways disease.
Conflict of interest statement
Ethics approval and consent to participate
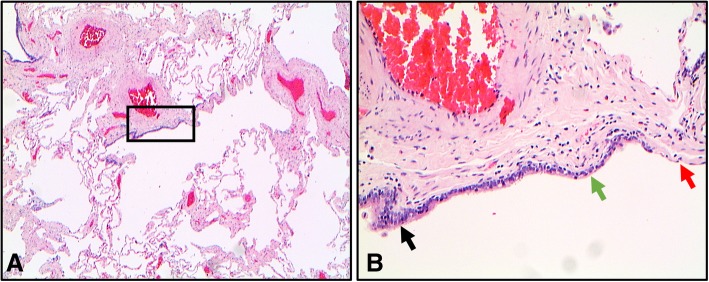
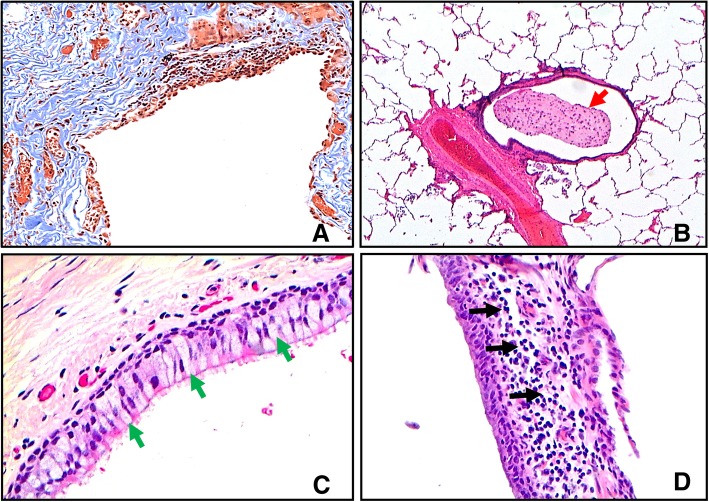
Tissue used to produce images in this review was taken from patients undergoing surgical resection for suspected lung cancer. All subjects gave written informed consent and this research was approved by the NRES Committee North West-Greater Manchester South (reference 03/SM/396).
Competing interests
AH has no competing interests. AMQ has received honoraria for lecturing for AstraZeneca and Roche and has acted as an advisor for Diaceutics Limited. DS has received sponsorship to attend international meetings, honoraria for lecturing or attending advisory boards and research grants from various pharmaceutical companies including Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Genentech, GlaxoSmithKline, Glenmark, Johnson and Johnson, Merck, NAPP, Novartis, Pfizer, Skypharma, Takeda, Teva, Therevance and Verona. JEDC has received sponsorship to attend international meetings, honoraria for lecturing or attending advisory boards from various pharmaceutical companies including Aché, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis and Pfizer.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Eur Respir J. 2017;49(3). - PubMed
-
- Weibel ER. Morphometry of the human lung. New York: Academic Press Inc.; 1963. pp. 110–135.
-
- Laennec R. Traité de l’auscultation médiate et des maladies des poumons et du coeur. New York: Samuel S and William Wood; 1819.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
