

Is early detection of late-onset Pompe disease a pneumologist's affair? A lesson from an Italian screening study
- PMID: 30832705
- PMCID: PMC6399888
- DOI: 10.1186/s13023-019-1037-1
Is early detection of late-onset Pompe disease a pneumologist's affair? A lesson from an Italian screening study
Abstract
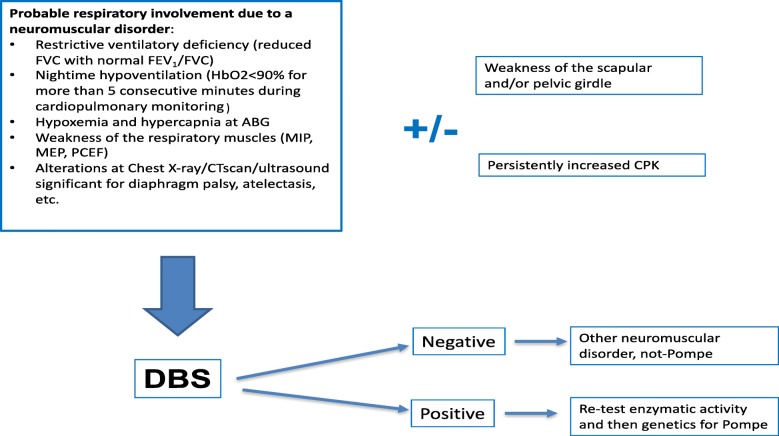
Background: Late-onset Pompe disease (LOPD) is a recessive disease caused by α-glucosidase (GAA) deficiency, leading to progressive muscle weakness and/or respiratory failure in children and adults. Respiratory derangement can be the first indication of LOPD, but the diagnosis may be difficult for pneumologists. We hypothesize that assessing the GAA activity in suspected patients by a dried blood spot (DBS) may help the diagnosis of LOPD in the pneumological setting.
Population and methods: We performed a multicenter DBS survey of patients with suspected LOPD according to a predefined clinical algorithm. From February 2015 to December 2017, 140 patients (57 ± 16 yrs., 80 males) were recruited in 19 Italian pneumological units. The DBS test was performed by a drop of blood collected on absorbent paper. Patients with GAA activity < 2.6 μmol/L/h were considered positive. A second DBS test was performed in the patients positive to the first assay. Patients testing positive at the re-test underwent a skeletal muscle biopsy to determine the GAA enzymatic activity.
Results: 75 recruited subjects had outpatient access, 65 subjects were admitted for an acute respiratory failure episode. Two patients tested positive in both the first and second DBS test (1.4% prevalence), and the LOPD diagnosis was confirmed through histology, with patients demonstrating a deficient GAA muscle activity (3.6 and 9.1 pmol/min/mg). A further five subjects were positive in the first DBS test but were not confirmed at re-test. The two positive cases were both diagnosed after hospitalization for acute respiratory failure and need of noninvasive ventilation. Most of the recruited patients had reduced maximal respiratory pressures (MIP 50 ± 27% and MEP 55 ± 27% predicted), restrictive pattern (FEV1/FVC 81.3 ± 13.6) and hypoxaemia (PaO2 70.9 ± 14.5 mmHg). Respiratory symptoms were present in all the patients, but only 48.6% of them showed muscle weakness in the pelvic girdle and/or in the scapular girdle (35.7%).
Conclusions: DBS GAA activity test may be a powerful screening tool among pneumologists, particularly in the acute setting. A simple clinical algorithm may aid in the selection of patients on which to administer the DBS test.
Keywords: Acute respiratory failure; Diagnosis; Late-onset Pompe disease; Noninvasive ventilation; Respiratory high dependency care unit.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was given by the C.E.R.U. Friuli-Venezia Giulia (ref.# 67/2014).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Winkel LP, Hagemans ML, Van Doorn PA, Loonen MC, Hop WJ, Reuser AJ, et al. The natural course of non-classic Pompe’s disease; a review of 225 published cases. J Neurol. 2005;252:875–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
