

Development of a multivariable gene-expression signature targeting T-cell-mediated rejection in peripheral blood of kidney transplant recipients validated in cross-sectional and longitudinal samples
- PMID: 30833191
- PMCID: PMC6441872
- DOI: 10.1016/j.ebiom.2019.01.060
Development of a multivariable gene-expression signature targeting T-cell-mediated rejection in peripheral blood of kidney transplant recipients validated in cross-sectional and longitudinal samples
Abstract
Background: Acute T-cell mediated rejection (TCMR) is usually indicated by alteration in serum-creatinine measurements when considerable transplant damage has already occurred. There is, therefore, a need for non-invasive early detection of immune signals that would precede the onset of rejection, prior to transplant damage.
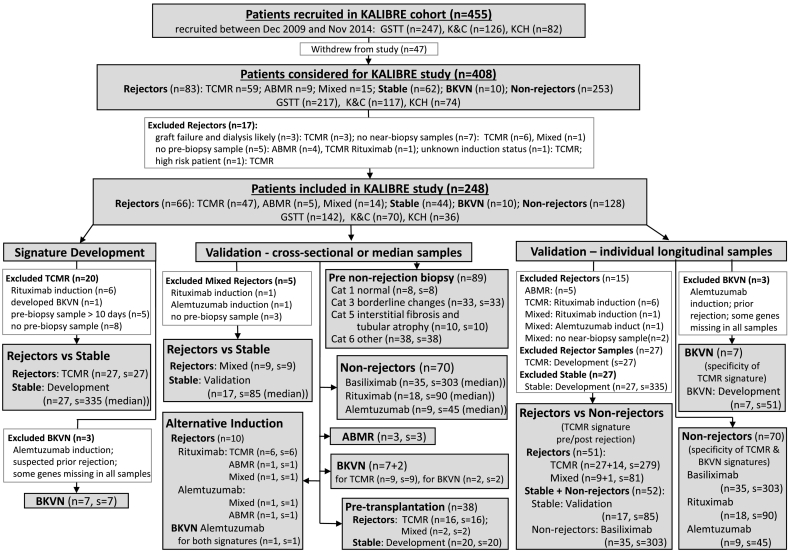
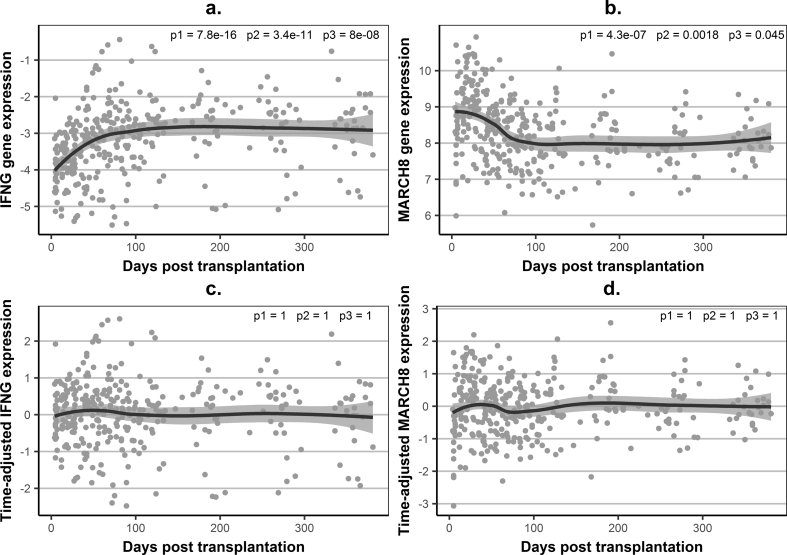
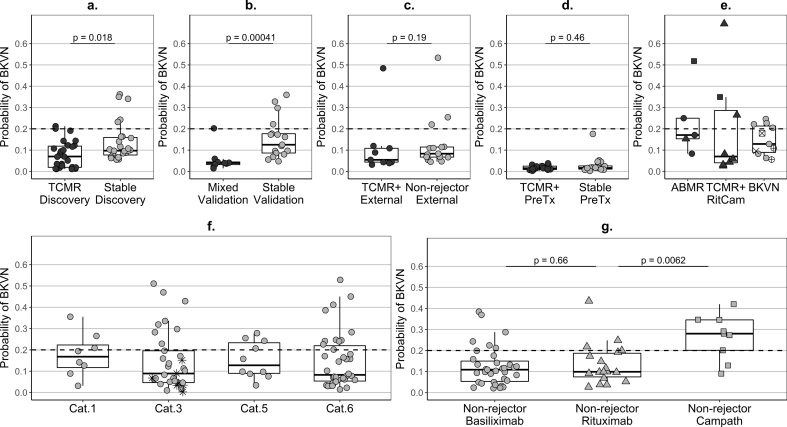
Methods: We examined the RT-qPCR expression of 22 literature-based genes in peripheral blood samples from 248 patients in the Kidney Allograft Immune Biomarkers of Rejection Episodes (KALIBRE) study. To account for post-transplantation changes unrelated to rejection, we generated time-adjusted gene-expression residuals from linear mixed-effects models in stable patients. To select genes, we used penalised logistic regression based on 27 stable patients and 27 rejectors with biopsy-proven T-cell-mediated rejection, fulfilling strict inclusion/exclusion criteria. We validated this signature in i) an independent group of stable patients and patients with concomitant T-cell and antibody-mediated-rejection, ii) patients from an independent study, iii) cross-sectional pre-biopsy samples from non-rejectors and iv) longitudinal follow-up samples covering the first post-transplant year from rejectors, non-rejectors and stable patients.
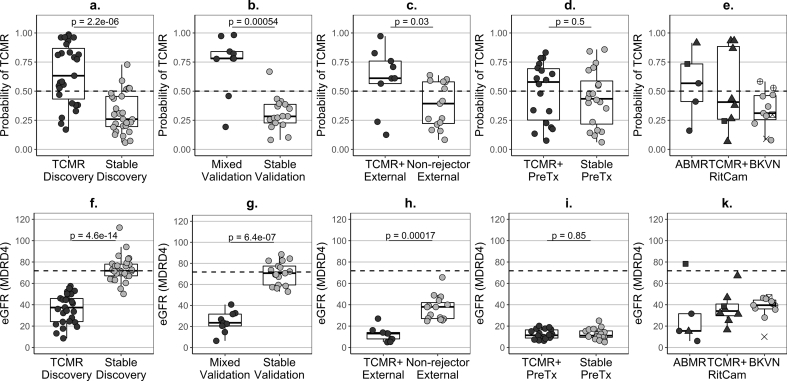
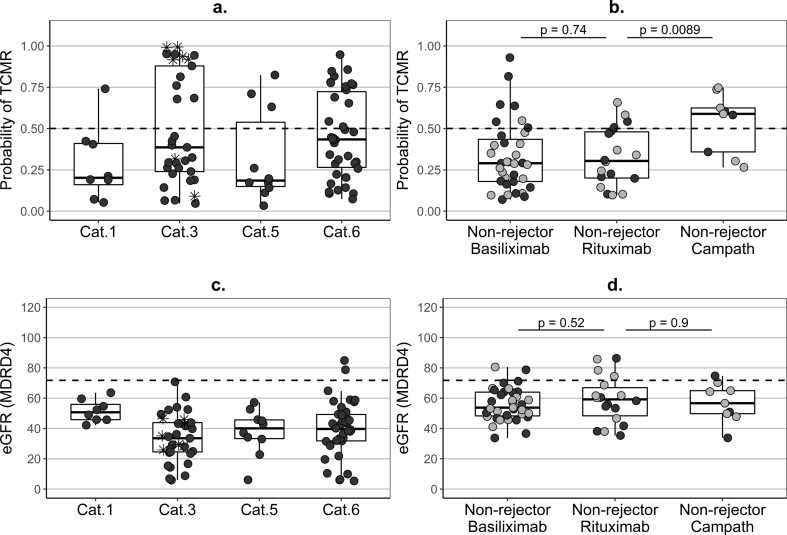
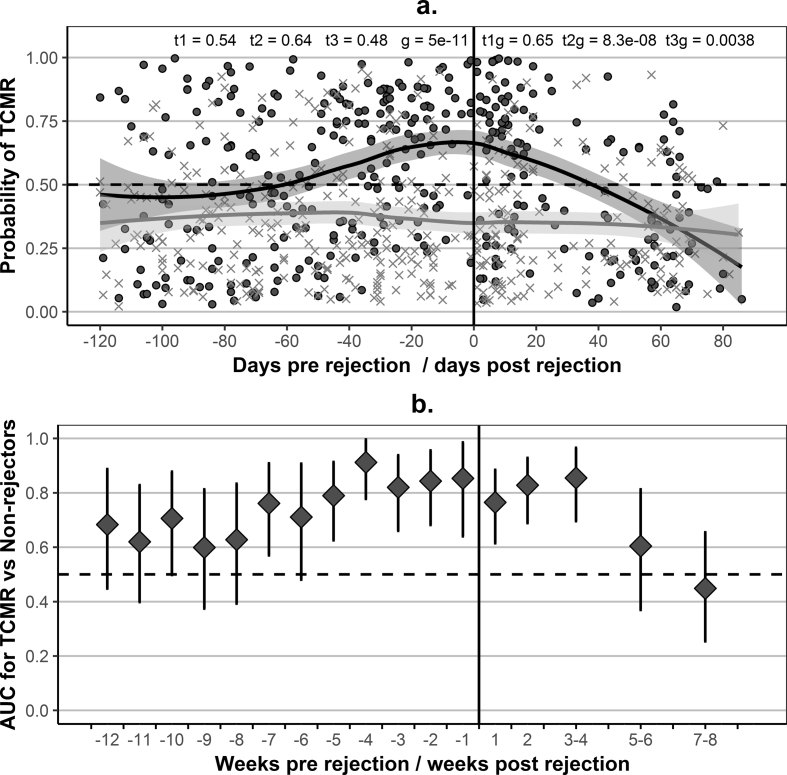
Findings: A parsimonious TCMR-signature (IFNG, IP-10, ITGA4, MARCH8, RORc, SEMA7A, WDR40A) showed cross-validated area-under-ROC curve 0.84 (0.77-0.88) (median, 2.5th-97.5th centile of fifty cross-validation cycles), sensitivity 0.67 (0.59-0.74) and specificity 0.85 (0.75-0.89). The estimated probability of TCMR increased seven weeks prior to the diagnostic biopsy and decreased after treatment. Gene expression in all patients showed pronounced variability, with up to 24% of the longitudinal samples in stable patients being TCMR-signature positive. In patients with borderline changes, up to 40% of pre-biopsy samples were TCMR-signature positive.
Interpretation: Molecular marker alterations in blood emerge well ahead of the time of clinically overt TCMR. Monitoring a TCMR-signature in peripheral blood could unravel T-cell-related pro-inflammatory activity and hidden immunological processes. This additional information could support clinical management decisions in cases of patients with stable but poor kidney function or with inconclusive biopsy results.
Copyright © 2019. Published by Elsevier B.V.
Figures
References
-
- Hoffmann S.C., Hale D.A., Kleiner D.E. Functionally significant renal allograft rejection is defined by transcriptional criteria. Am J Transplant. 2005;5(3):573–581. - PubMed
-
- Deng M.C. The AlloMap genomic biomarker story: 10 years after. Clin Transplant. 2017;31(3) - PubMed
-
- Bohl D.L., Brennan D.C. BK Virus Nephropathy and Kidney Transplantation. Clin J Am Soc Nephrol. 2007;2(Supplement 1):S36–S46. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
