

External Evaluation of Population Pharmacokinetic Models of Vancomycin in Large Cohorts of Intensive Care Unit Patients
- PMID: 30833424
- PMCID: PMC6496102
- DOI: 10.1128/AAC.02543-18
External Evaluation of Population Pharmacokinetic Models of Vancomycin in Large Cohorts of Intensive Care Unit Patients
Abstract
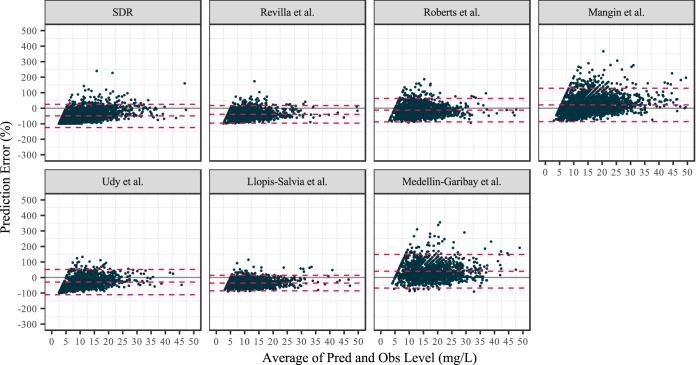
Dosing of vancomycin is often guided by therapeutic drug monitoring and population pharmacokinetic models in the intensive care unit (ICU). The validity of these models is crucial, as ICU patients have marked pharmacokinetic variability. Therefore, we set out to evaluate the predictive performance of published population pharmacokinetic models of vancomycin in ICU patients. The PubMed database was used to search for population pharmacokinetic models of vancomycin in adult ICU patients. The identified models were evaluated in two independent data sets which were collected from two large hospitals in the Netherlands (Amsterdam UMC, Location VUmc, and OLVG Oost). We also tested a one-compartment model with fixed values for clearance and volume of distribution, in which a clinical standard dosage regimen (SDR) was mimicked to assess its predictive performance. Prediction error was calculated to assess the predictive performance of the models. Six models plus the SDR model were evaluated. The model of Roberts et al. (J. A. Roberts, F. S. Taccone, A. A. Udy, J.-L. Vincent, F. Jacobs, and J. Lipman, Antimicrob Agents Chemother 55:2704-2709, 2011, https://doi.org/10.1128/AAC.01708-10) performed satisfactorily, with mean and median values of prediction error of 5.1% and -7.5%, respectively, for Amsterdam UMC, Location VUmc, patients, and -12.6% and -17.2% respectively, for OLVG Oost patients. The other models, including the SDR model, yielded high mean values (-49.7% to 87.7%) and median values (-56.1% to 66.1%) for both populations. In conclusion, only the model of Roberts et al. was able to validly predict the concentrations of vancomycin for our data, whereas other models and standard dosing were largely inadequate. Extensive evaluation should precede the adoption of any model in clinical practice for ICU patients.
Keywords: ICU patients; NONMEM; antibiotics; model validation; population pharmacokinetics; vancomycin.
Copyright © 2019 American Society for Microbiology.
Figures


References
-
- Rybak M, Lomaestro B, Rotschafer JC, Moellering R, Craig W, Billeter M, Dalovisio JR, Levine DP, Reilly C. 2009. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm 66:82–98. doi: 10.2146/ajhp080434. - DOI - PubMed
-
- Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, Rybak MJ, Talan DA, Chambers HF, Infectious Diseases Society of America. 2011. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis 52:e18–e55. doi: 10.1093/cid/ciq146. - DOI - PubMed
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche J-D, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent J-L, Angus DC. 2016. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
