

Association between Nonalcoholic Fatty Liver Disease at CT and Coronary Microvascular Dysfunction at Myocardial Perfusion PET/CT
- PMID: 30835188
- PMCID: PMC6492883
- DOI: 10.1148/radiol.2019181793
Association between Nonalcoholic Fatty Liver Disease at CT and Coronary Microvascular Dysfunction at Myocardial Perfusion PET/CT
Abstract
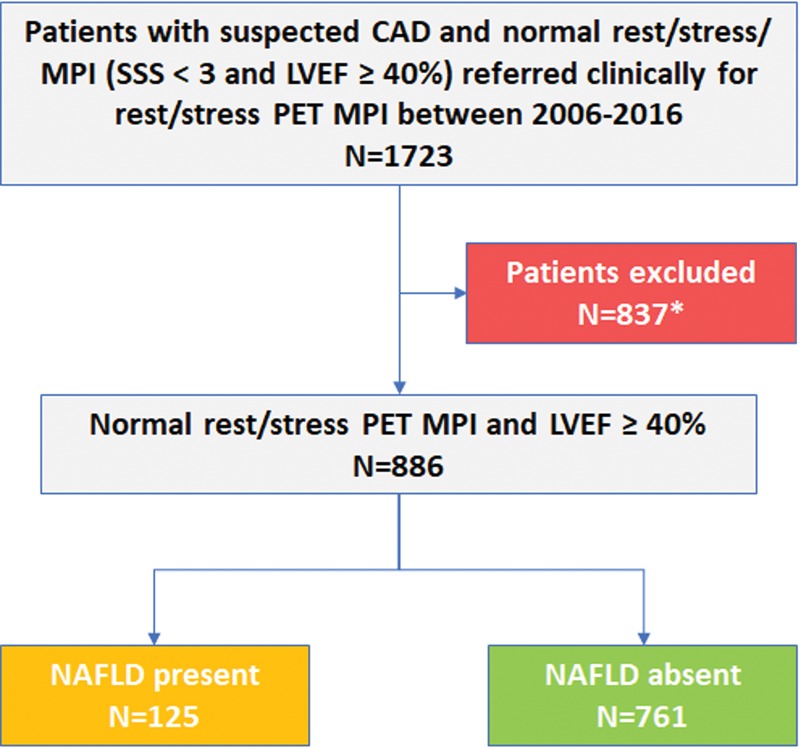
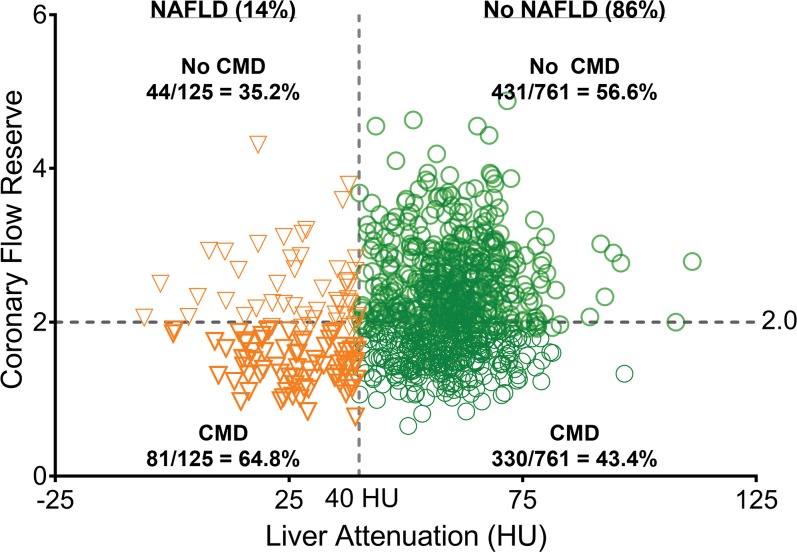
Background Cardiovascular disease is a major cause of mortality in patients with nonalcoholic fatty liver disease (NAFLD). However, the association of NAFLD with coronary microvascular dysfunction is, to our knowledge, unknown. Purpose To determine whether coronary microvascular dysfunction is more prevalent in patients with NAFLD and to determine whether coronary microvascular dysfunction predicts major adverse cardiac events (MACE) independently of NAFLD. Materials and Methods This retrospective study (2006-2014) included patients without evidence of obstructive epicardial coronary artery disease and healthy left ventricular ejection fraction (≥40%) at a clinical rest and stress myocardial perfusion PET/CT. NAFLD was defined by a mean hepatic attenuation of less than 40 HU at CT and coronary microvascular dysfunction as a coronary flow reserve (CFR) of less than 2.0. A composite of all-cause mortality, myocardial infarction, coronary revascularization, and hospitalization because of heart failure comprised MACE (130 of 886 patients; 14.7%). The relation between NAFLD and MACE was assessed by using multivariable Cox regression analysis. Results Among 886 patients (mean age, 62 years ± 12 [standard deviation]; 631 women [mean age, 62 years ± 12 years] and 255 men [mean age, 61 years ± 12]; and ejection fraction, 63% ± 9), 125 patients (14.1%) had NAFLD and 411 patients (46.4%) had coronary microvascular dysfunction. Coronary microvascular dysfunction was more prevalent (64.8% vs 43.4%; P < .001) and CFR was lower (1.9 ± 1.1 vs 2.2 ± 0.7; P < .001) in patients with NAFLD compared with those without NAFLD. NAFLD independently predicted coronary microvascular dysfunction (P = .01). The interaction of NAFLD and male sex predicted MACE (hazard ratio, 1.45; 95% confidence interval: 1.08, 1.69; P = .008) and coronary microvascular dysfunction remained associated with MACE (adjusted hazard ratio, 1.46; 95% confidence interval: 1.02, 2.07; P = .04). Conclusion Coronary microvascular dysfunction was more prevalent in patients with nonalcoholic fatty liver disease and predicted major adverse cardiac events independently of nonalcoholic fatty liver disease. © RSNA, 2019 Online supplemental material is available for this article. See also the editorial by Ambale-Venkatesh and Lima in this issue.
Figures
Comment in
-
Probing the Liver-Heart Axis.Radiology. 2019 May;291(2):338-339. doi: 10.1148/radiol.2019190264. Epub 2019 Mar 5. Radiology. 2019. PMID: 30835190 No abstract available.
References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64(1):73–84. - PubMed
-
- Chalasani N, Younossi Z, Lavine JE, et al. . The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018;67(1):328–357. - PubMed
-
- Adams LA, Anstee QM, Tilg H, Targher G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017;66(6):1138–1153. - PubMed
-
- Després JP, Lamarche B, Mauriège P, et al. . Hyperinsulinemia as an independent risk factor for ischemic heart disease. N Engl J Med 1996;334(15):952–957. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
