

Dose Escalation for Prostate Adenocarcinoma: A Long-Term Update on the Outcomes of a Phase 3, Single Institution Randomized Clinical Trial
- PMID: 30836166
- PMCID: PMC6579684
- DOI: 10.1016/j.ijrobp.2019.02.045
Dose Escalation for Prostate Adenocarcinoma: A Long-Term Update on the Outcomes of a Phase 3, Single Institution Randomized Clinical Trial
Abstract
Purpose: To determine the long-term outcomes for prostate adenocarcinoma when escalating radiation dose from 70 Gy to 78 Gy.
Methods and materials: Between 1993 and 1998, 301 patients with biopsy-proven clinical stage T1b-T3 prostate adenocarcinoma, any prostate-specific antigen level, and any Gleason score were randomized to 70 Gy in 35 fractions versus 78 Gy in 39 fractions of photon radiation therapy using a 4-field box technique without hormone deprivation therapy. The primary outcome was powered to detect a 15% difference in biochemical or clinical failure. Secondary outcomes included survival, prostate cancer mortality, biochemical failure, local failure, nodal failure, distant failure, and secondary malignancy rates.
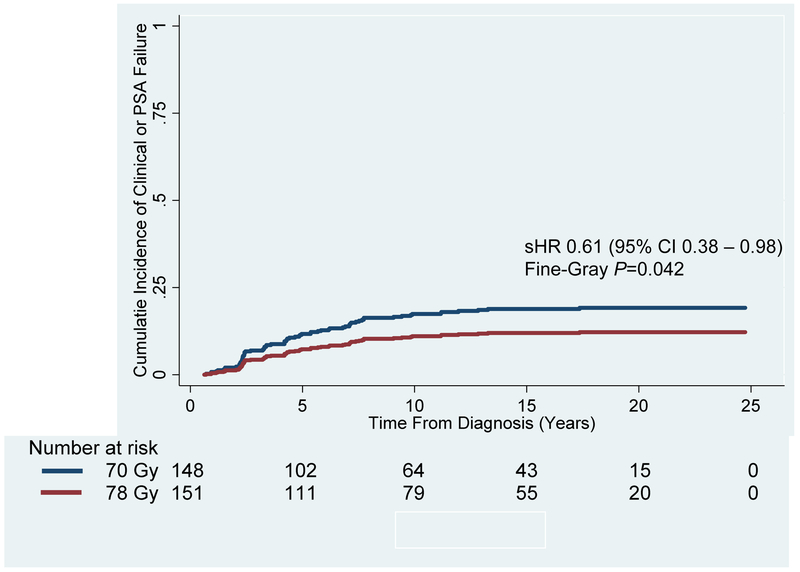
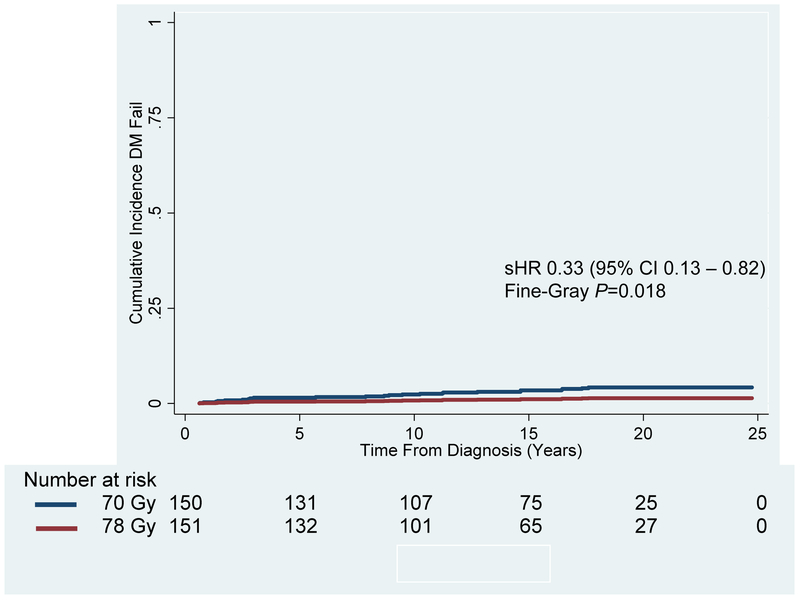
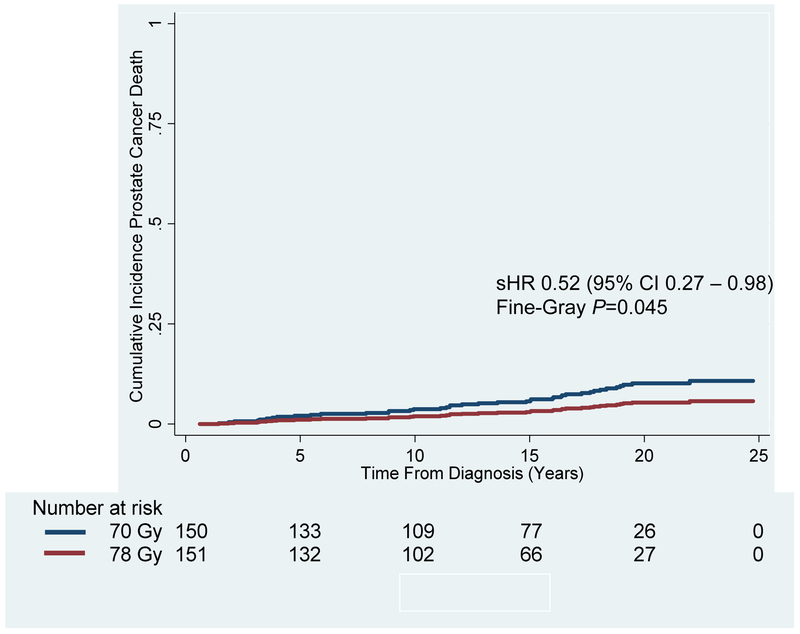
Results: With a median follow-up of 14.3 years, the cumulative incidence of 15-year biochemical or clinical failure was 18.9% versus 12.0% in the 70 Gy versus 78 Gy arms, respectively (subhazard ratio [sHR], 0.61; 95% confidence interval [CI], 0.38-0.98; Fine-Gray P = .042). The 15-year cumulative incidence of distant metastasis was 3.4% versus 1.1%, respectively (sHR, 0.33; 95% CI, 0.13-0.82; Fine-Gray P = .018). The 15-year cumulative incidence of prostate cancer-specific mortality was 6.2% versus 3.2%, respectively, (sHR, 0.52; 95% CI, 0.27-0.98; Fine-Gray P = .045). There were no differences in overall survival (HR, 1.10; 95% CI, 0.84-1.45; log rank P = .469) or other-cause survival (sHR, 1.33; 95% CI, 0.99-1.79; Fine-Gray P = .061). Salvage therapy was more common in the 70 Gy arm, at 38.7% versus 21.9% in the 78 Gy arm (P = .002). There was a 2.3% secondary solid malignancy rate (1 bladder, 6 rectal) within the radiation treatment field, which was not significantly different between treatment arms.
Conclusions: Dose escalation by 8 Gy (78 Gy vs 70 Gy) provided a sustained improvement in biochemical and clinical failure, which translated into lower salvage rates and improved prostate cancer-specific mortality, but not overall survival. Long-term follow-up demonstrated a low incidence of potential solid tumor secondary malignancies.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Long-Term Benefits of Dose-Escalation in Localized Prostate Cancer.Int J Radiat Oncol Biol Phys. 2019 Jul 15;104(4):798-800. doi: 10.1016/j.ijrobp.2019.04.001. Int J Radiat Oncol Biol Phys. 2019. PMID: 31204661 No abstract available.
References
-
- Wang JZ, Guerrero M, and Li XA, How low is the alpha/beta ratio for prostate cancer? Int J Radiat Oncol Biol Phys, 2003. 55(1): p. 194–203. - PubMed
-
- Pollack A, Smith LG, and von Eschenbach AC, External beam radiotherapy dose response characteristics of 1127 men with prostate cancer treated in the PSA era. Int J Radiat Oncol Biol Phys, 2000. 48(2): p. 507–12. - PubMed
-
- Beckendorf V, et al. , 70 Gy versus 80 Gy in localized prostate cancer: 5-year results of GETUG 06 randomized trial. Int J Radiat Oncol Biol Phys, 2011. 80(4): p. 1056–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
