

Gonorrhoea and chlamydia diagnosis as an entry point for HIV pre-exposure prophylaxis: a modelling study
- PMID: 30837248
- PMCID: PMC6429744
- DOI: 10.1136/bmjopen-2018-023453
Gonorrhoea and chlamydia diagnosis as an entry point for HIV pre-exposure prophylaxis: a modelling study
Abstract
Objectives: Neisseria gonorrhoeae (NG) and Chlamydia trachomatis (CT) increase the risk of HIV transmission among men who have sex with men (MSM). Diagnosis of NG/CT may provide an efficient entry point for prevention of HIV through the delivery of pre-exposure prophylaxis (PrEP); however, the additional population-level impact of targeting PrEP to MSM diagnosed with NG/CT is unknown.
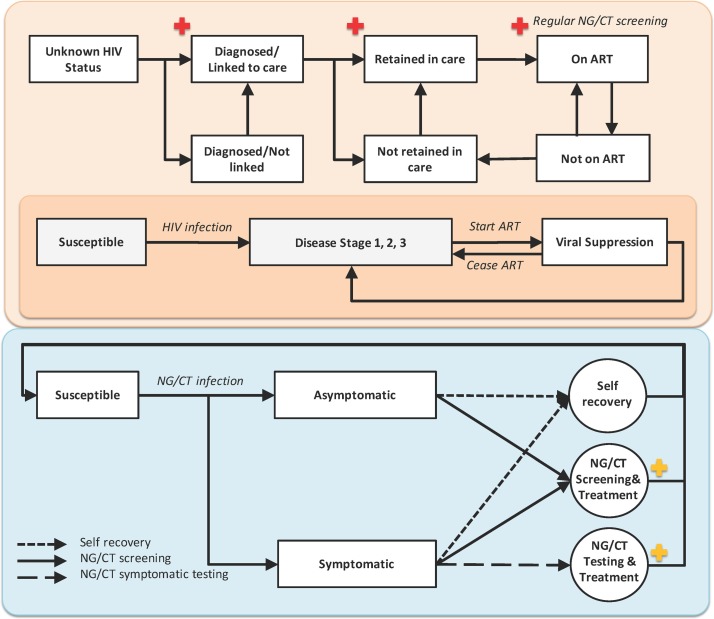
Design: An agent-based simulation model of NG/CT and HIV cocirculation among MSM calibrated against census data, disease surveillance reports and the US National HIV Behavioral Surveillance study.
Setting: Baltimore City, Maryland, USA.
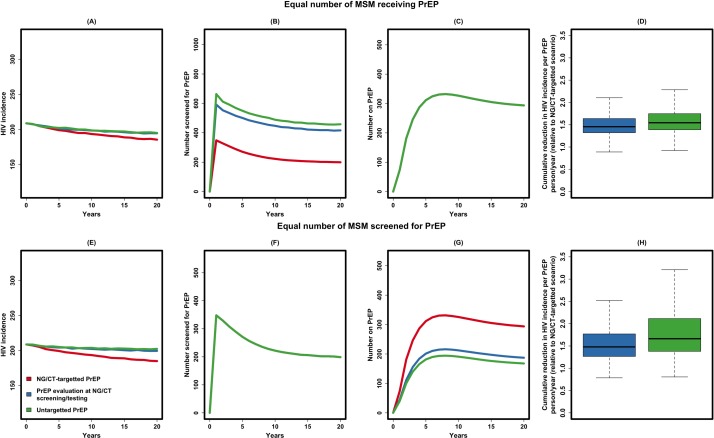
Interventions: PrEP implementation was modelled under three alternative scenarios: (1) PrEP delivery at NG/CT diagnosis (targeted delivery), (2) PrEP evaluation at NG/CT screening/testing and (3) PrEP evaluation in the general community (untargeted).
Main outcome: The projected incidence of HIV after 20 years of PrEP delivery under two alternatives: when equal numbers of MSM are (1) screened for PrEP or (2) receive PrEP in each year.
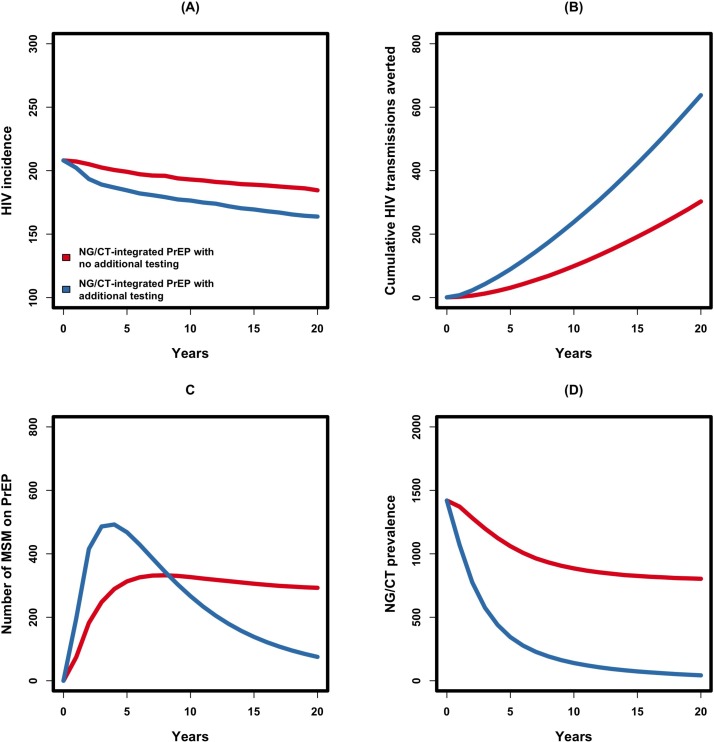
Results: Assuming 60% uptake and 60% adherence, targeting PrEP to MSM diagnosed with NG/CT could reduce HIV incidence among MSM in Baltimore City by 12.4% (95% uncertainty range (UR) 10.3% to 14.4%) in 20 years, relative to no PrEP. Expanding the coverage of NG/CT screening (such that individuals experience a 50% annual probability of NG/CT screening and evaluation for PrEP on NG/CT diagnosis) can further increase the impact of targeted PrEP to generate a 22.0% (95% UR 20.1% to 23.9%) reduction in HIV incidence within 20 years. When compared with alternative implementation scenarios, PrEP evaluation at NG/CT diagnosis increased impact of PrEP on HIV incidence by 1.5(95% UR 1.1 to 1.9) times relative to a scenario in which PrEP evaluation happened at the time of NG/CT screening/testing and by 1.6 (95% UR 1.2 to 2.2) times relative to evaluating random MSM from the community.
Conclusions: Targeting MSM infected with NG/CT increases the efficiency and effectiveness of PrEP delivery. If high levels of sexually transmitted infection screening can be achieved at the community level, NG/CT diagnosis may be a highly effective entry point for PrEP initialisation.
Keywords: Hiv Infection; chlamydia; computer simulation; gonorrhea; homosexuality; pre-exposure prophylaxis.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
STI in times of PrEP: high prevalence of chlamydia, gonorrhea, and mycoplasma at different anatomic sites in men who have sex with men in Germany.BMC Infect Dis. 2020 Feb 7;20(1):110. doi: 10.1186/s12879-020-4831-4. BMC Infect Dis. 2020. PMID: 32033533 Free PMC article.
-
Sexually Transmitted Infection Screening Among Gay, Bisexual, and Other Men Who Have Sex With Men Prescribed Pre-exposure Prophylaxis in Baltimore City, Maryland.Clin Infect Dis. 2020 Dec 17;71(10):2637-2644. doi: 10.1093/cid/ciz1145. Clin Infect Dis. 2020. PMID: 31761944
-
Impact of Providing Preexposure Prophylaxis for Human Immunodeficiency Virus at Clinics for Sexually Transmitted Infections in Baltimore City: An Agent-based Model.Sex Transm Dis. 2018 Dec;45(12):791-797. doi: 10.1097/OLQ.0000000000000882. Sex Transm Dis. 2018. PMID: 29944642 Free PMC article.
-
Sexually transmitted infections and pre-exposure prophylaxis: challenges and opportunities among men who have sex with men in the US.AIDS Res Ther. 2016 Jan 19;13:5. doi: 10.1186/s12981-016-0089-8. eCollection 2016. AIDS Res Ther. 2016. PMID: 26793265 Free PMC article. Review.
-
Screening is not associated with reduced incidence of gonorrhoea or chlamydia in men who have sex with men (MSM); an ecological study of 23 European countries.F1000Res. 2019 Feb 6;8:160. doi: 10.12688/f1000research.17955.2. eCollection 2019. F1000Res. 2019. PMID: 31543953 Free PMC article. Review.
Cited by
-
Knowledge domain and emerging trends in HIV pre-exposure prophylaxis: A visualization analysis via CiteSpace.Front Microbiol. 2023 Mar 16;14:1099132. doi: 10.3389/fmicb.2023.1099132. eCollection 2023. Front Microbiol. 2023. PMID: 37007528 Free PMC article.
-
Diagnostic Tests for Detecting Chlamydia trachomatis and Neisseria gonorrhoeae in Rectal and Pharyngeal Specimens.J Clin Microbiol. 2022 Apr 20;60(4):e0021121. doi: 10.1128/JCM.00211-21. Epub 2021 Nov 3. J Clin Microbiol. 2022. PMID: 34731021 Free PMC article. Review.
-
Acceptability of Multilevel Sexual Health Interventions and Sexually Transmitted Infection Screening and Testing Among Persons With HIV Across Three Clinical Sites in Florida.J Acquir Immune Defic Syndr. 2025 Mar 1;98(3):282-290. doi: 10.1097/QAI.0000000000003569. Epub 2025 Feb 5. J Acquir Immune Defic Syndr. 2025. PMID: 39813221 Free PMC article.
-
Routine testing for chlamydia and gonorrhea in an HIV preexposure prophylaxis program in Hanoi, Vietnam: implications for low- and middle-income countries.AIDS. 2025 Jul 15;39(9):1152-1160. doi: 10.1097/QAD.0000000000004203. Epub 2025 Apr 3. AIDS. 2025. PMID: 40334065
-
Cross-sectional assessment of determinants of STIs among men who have sex with men and transgender women in Kigali, Rwanda.Sex Transm Infect. 2022 May;98(3):178-187. doi: 10.1136/sextrans-2020-054753. Epub 2021 May 6. Sex Transm Infect. 2022. PMID: 33958492 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous