

Reduced vs. standard dose native E. coli-asparaginase therapy in childhood acute lymphoblastic leukemia: long-term results of the randomized trial Moscow-Berlin 2002
- PMID: 30840197
- PMCID: PMC6435612
- DOI: 10.1007/s00432-019-02854-x
Reduced vs. standard dose native E. coli-asparaginase therapy in childhood acute lymphoblastic leukemia: long-term results of the randomized trial Moscow-Berlin 2002
Abstract
Purpose: Favorable outcomes were achieved for children with acute lymphoblastic leukemia (ALL) with the first Russian multicenter trial Moscow-Berlin (ALL-MB) 91. One major component of this regimen included a total of 18 doses of weekly intramuscular (IM) native Escherichia coli-derived asparaginase (E. coli-ASP) at 10000 U/m2 during three consolidation courses. ASP was initially available from Latvia, but had to be purchased from abroad at substantial costs after the collapse of Soviet Union. Therefore, the subsequent trial ALL-MB 2002 aimed at limiting costs to a reasonable extent and also at reducing toxicity by lowering the dose for standard risk (SR-) patients to 5000 U/m2 without jeopardizing efficacy.
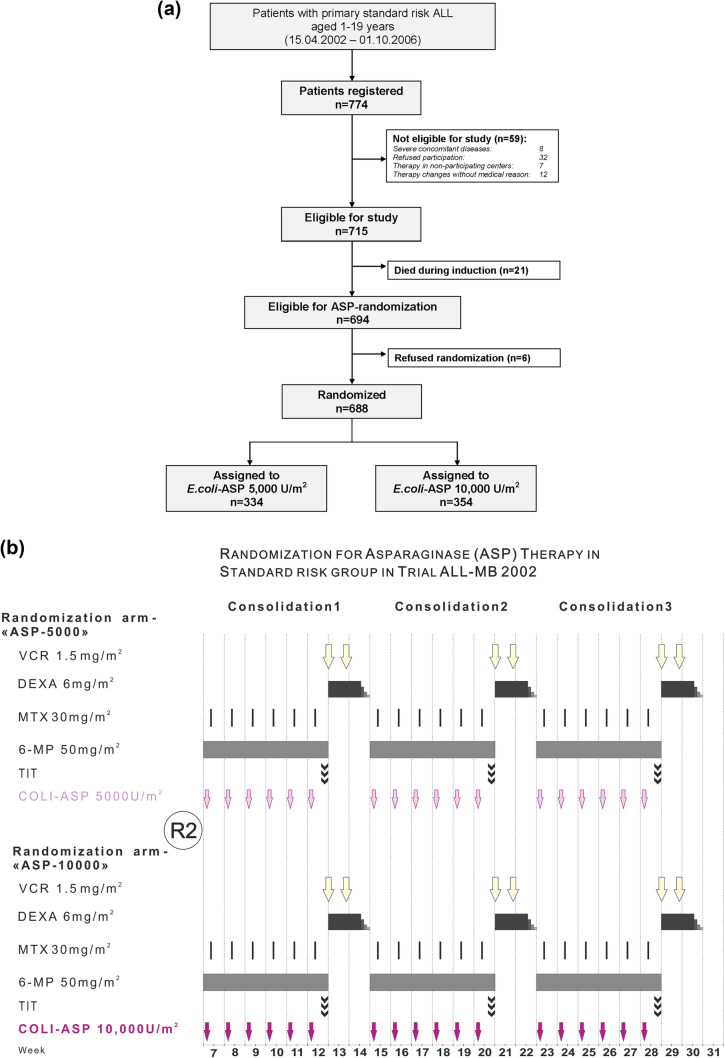
Methods: Between April 2002 and November 2006, 774 SR patients were registered in 34 centers across Russia and Belarus, 688 of whom were randomized. In arm ASP-5000 (n = 334), patients received 5000 U/m2 and in arm ASP-10000 (n = 354) 10 000 U/m2 IM.
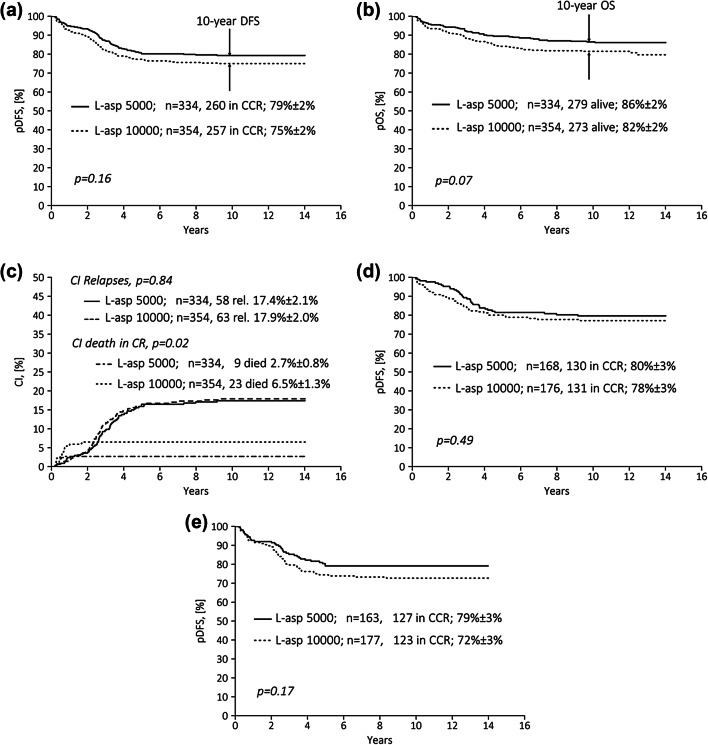
Results: Probabilities of disease-free survival, overall survival and cumulative incidence of relapse at 10 years were comparable: 79 ± 2%, 86 ± 2% and 17.4 ± 2.1% (ASP-5000) vs. 75 ± 2% and 82 ± 2%, and 17.9 ± 2.0% (ASP-10000), while death in complete remission was significantly lower in arm ASP-5000 (2.7% vs. 6.5%; p = 0.029).
Conclusion: Our findings suggest that weekly 5000 U/m2E. coli-ASP IM during consolidation therapy are equally effective, more cost-efficient and less toxic than 10000 U/m2 for SR patients with childhood ALL.
Keywords: Acute lymphoblastic leukemia; Children; Multicenter trial; Native Escherichia coli-derived asparaginase.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
