

MRI prognostic factors of tongue cancer: potential predictors of cervical lymph nodes metastases
- PMID: 30840589
- PMCID: PMC6411025
- DOI: 10.2478/raon-2019-0012
MRI prognostic factors of tongue cancer: potential predictors of cervical lymph nodes metastases
Abstract
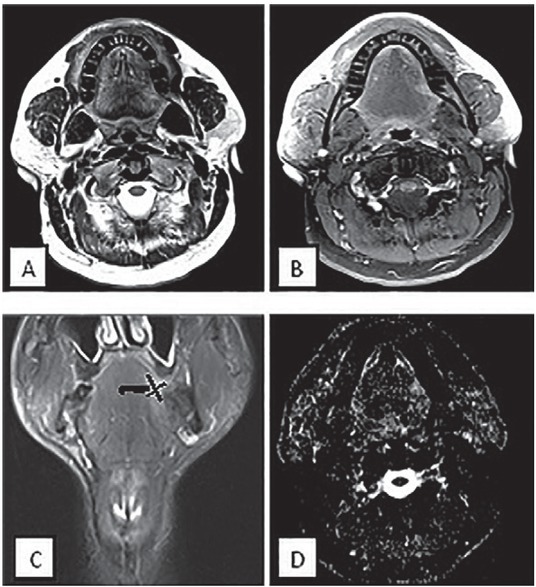
Background This study aimed to evaluate the efficacy of three MR imaging parameters, which are tumour thickness, para-lingual distance and apparent diffusion coefficient (ADC) value for prediction of cervical lymph nodes metastasis in cancer tongue patients. Patients and methods Fifty patients with proved cancer tongue by histopathological examination underwent MRI examination. T1 and T2- weighted MRI, diffusion-weighted images and post-contrast T1 fat suppression sequences were used. Results The patients were classified according to lymph nodes involvement as seen by MRI into two groups. Significant differences between positive and negative nodes groups were observed regarding tumour thickness and para-lingual distance (p-values = 0.008 and 0.003 respectively). ROC curve analyses revealed cut-off values >13.8 mm and ≤ 3.3 mm for tumour thickness and para-lingual distance respectively for prediction of nodes involvement. No significant differences between patients with and without cervical lymph nodes metastasis were found regarding corresponding ADC value of the tumour (p-value = 0.518). Conclusions Para-lingual distance and tumour thickness are factors that could influence pre-operative judgment and prognosis of tongue cancer patients. ADC value of the tumour itself seem not to be a reliable index of cancer progression to regional lymph nodes.
Keywords: apparent diffusion coefficient; cervical lymph nodes metastases; para-lingual distance; tongue cancer; tumour thickness.
Figures




References
-
- Funk GF, Karnell LH, Robinson RA, Zhen WK, Trask DK, Hoffman HT. Presentation, treatment, and outcome of oral cavity cancer: a National Cancer Data Base report. Head Neck. 2002;24:165–80. - PubMed
-
- Stone M, Davis EP, Douglas AS, Aiver MN, Gullapalli R, Levine WS. Modeling tongue surface contours from Cine-MRI images. J Speech Lang Hear Res. 2001;44:1026–40. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical