

Prevalence and Anatomy of Aberrant Right Subclavian Artery Evaluated by Computed Tomographic Angiography at a Single Institution in Korea
- PMID: 30840972
- PMCID: PMC6411572
- DOI: 10.3340/jkns.2018.0048
Prevalence and Anatomy of Aberrant Right Subclavian Artery Evaluated by Computed Tomographic Angiography at a Single Institution in Korea
Abstract
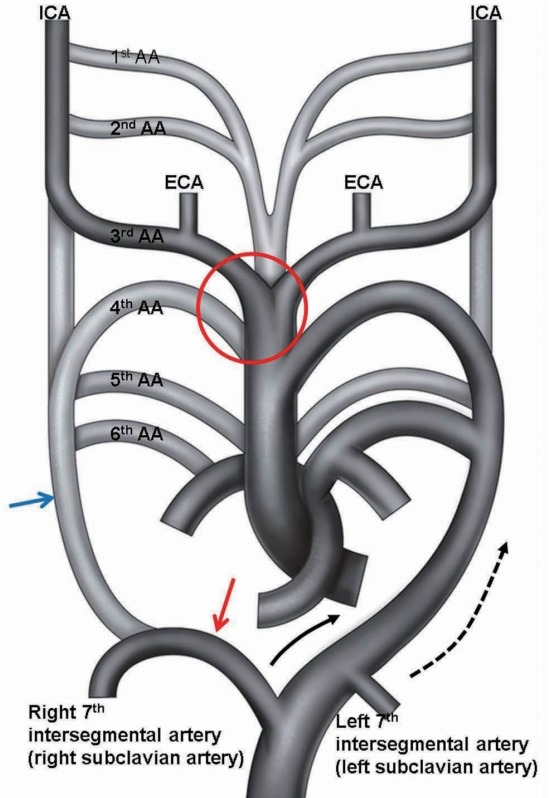
Objective: Aberrant right subclavian artery (ARSA) is a rare anatomical variant of the origin of the right subclavian artery. ARSA is defined as the right subclavian artery originating as the final branch of the aortic arch. The purpose of this study is to determine the prevalence and the anatomy of ARSA evaluated with computed tomography (CT) angiography.
Methods: CT angiography was performed in 3460 patients between March 1, 2014 and November 30, 2015 and the results were analyzed. The origin of the ARSA, course of the vessel, possible inadvertent ARSA puncture site during subclavian vein catheterization, Kommerell diverticula, and associated vascular anomalies were evaluated. We used the literature to review the clinical importance of ARSA.
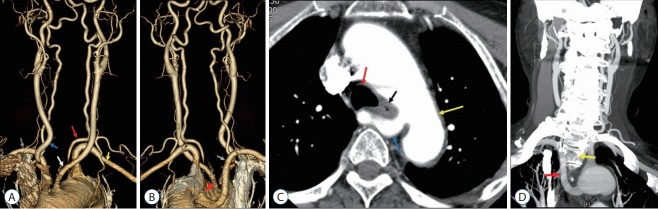
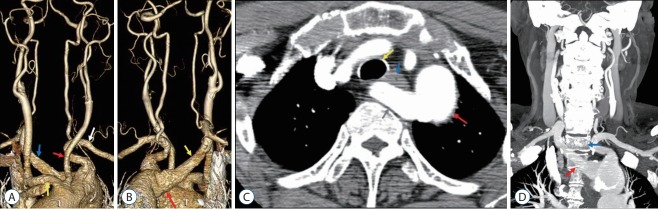
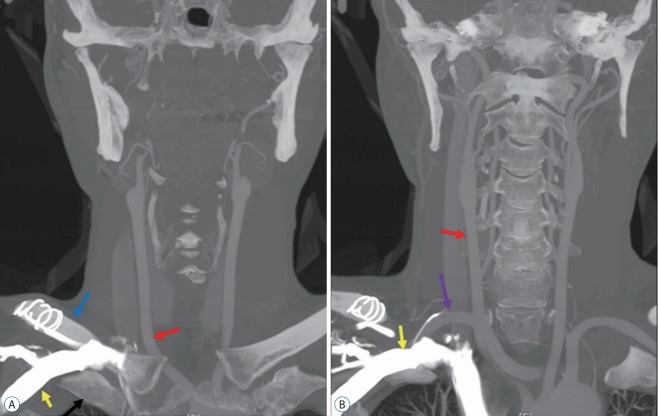
Results: Seventeen in 3460 patients had ARSA. All ARSAs in 17 patients originated from the posterior aspect of the aortic arch and traveled along a retroesophageal course to the right thoracic outlet. All 17 ARSAs were located in the anterior portion from first to fourth thoracic vertebral bodies and were located near the right subclavian vein at the medial third of the clavicle. Only one of 17 patients presented with dysphagia.
Conclusion: It is important to be aware ARSA before surgical approaches to upper thoracic vertebrae in order to avoid complications and effect proper treatment. In patients with a known ARSA, a right transradial approach for aortography or cerebral angiography should be changed to a left radial artery or transfemoral approach.
Keywords: Aberrant subclavian artery; Clinical; Computed tomography angiography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Backer CL, Ilbawi MN, Idriss FS, DeLeon SY. Vascular anomalies causing tracheoesophageal compression. Review of experience in children. J Thorac Cardiovasc Surg. 1989;97:725–731. - PubMed
-
- Bayford D. An account of singular case of obstructed deglutition. Mem Med Soc Lond. 1794;2:275–286.
-
- Berko NS, Jain VR, Godelman A, Stein EG, Ghosh S, Haramati LB. Variants and anomalies of thoracic vasculature on computed tomographic angiography in adults. J Comput Assist Tomogr. 2009;33:523–528. - PubMed
-
- Celikyay ZR, Koner AE, Celikyay F, Denız C, Acu B, Firat MM. Frequency and imaging findings of variations in human aortic arch anatomy based on multidetector computed tomography data. Clin Imaging. 2013;37:1011–1019. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
