

Activin type II receptor signaling in cardiac aging and heart failure
- PMID: 30842316
- PMCID: PMC7124007
- DOI: 10.1126/scitranslmed.aau8680
Activin type II receptor signaling in cardiac aging and heart failure
Abstract
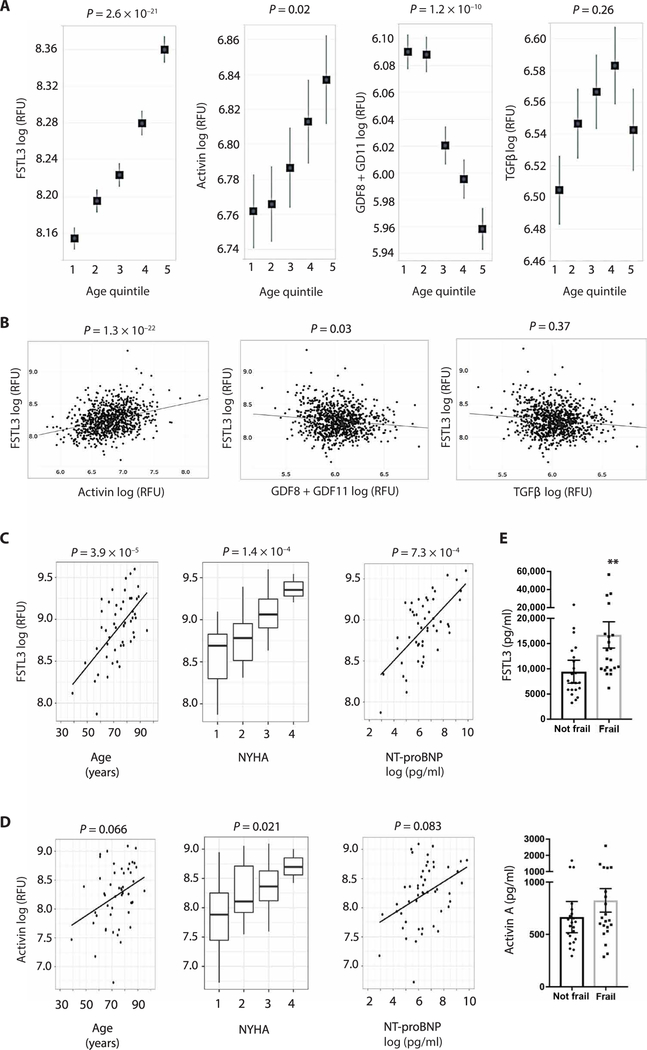
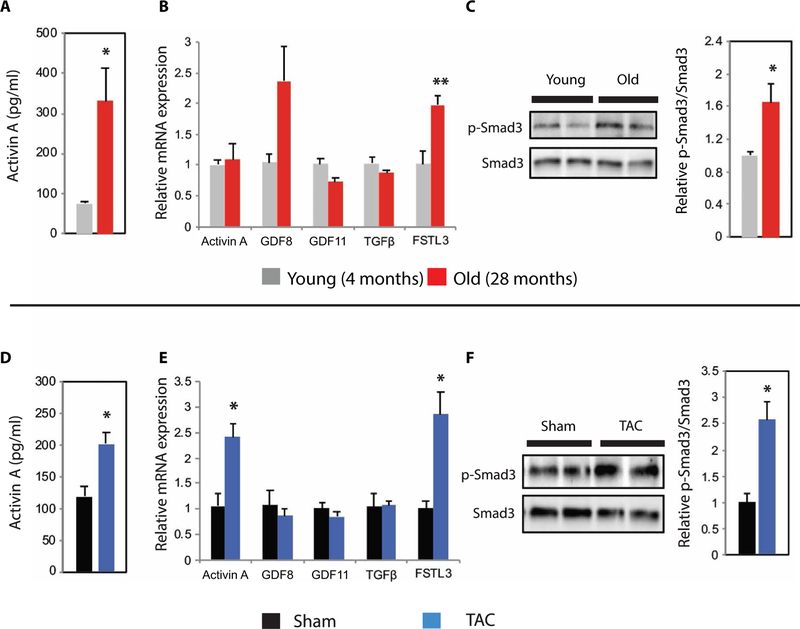
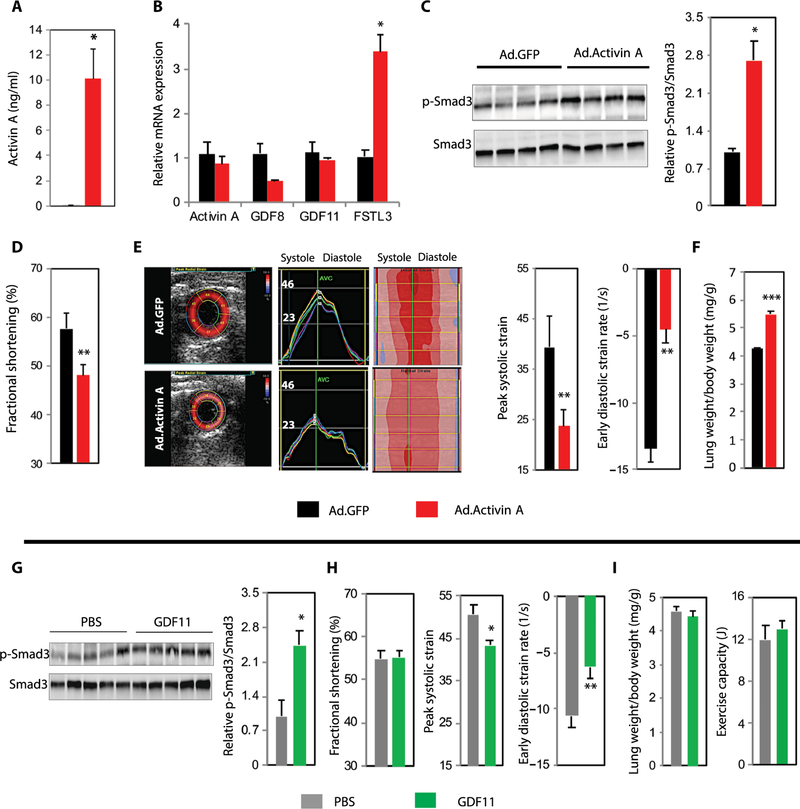
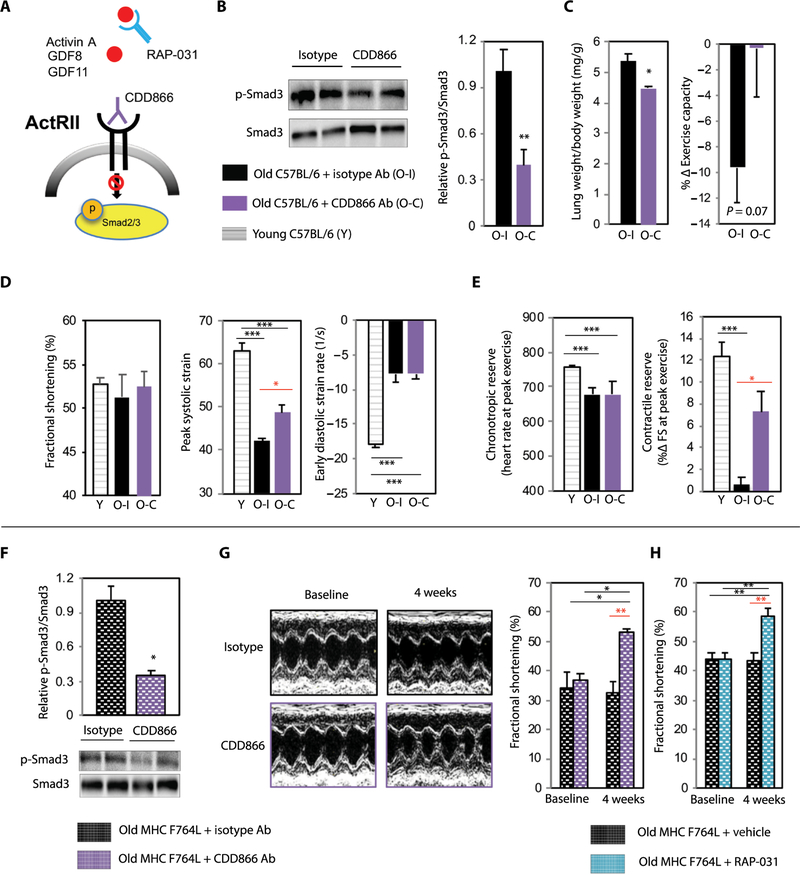
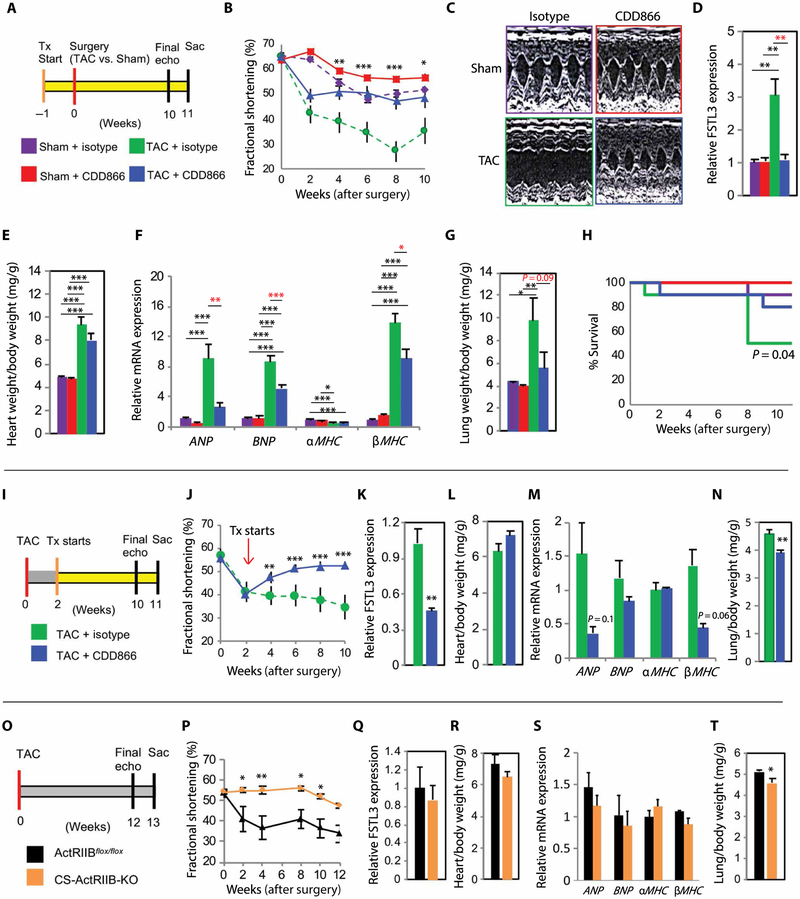
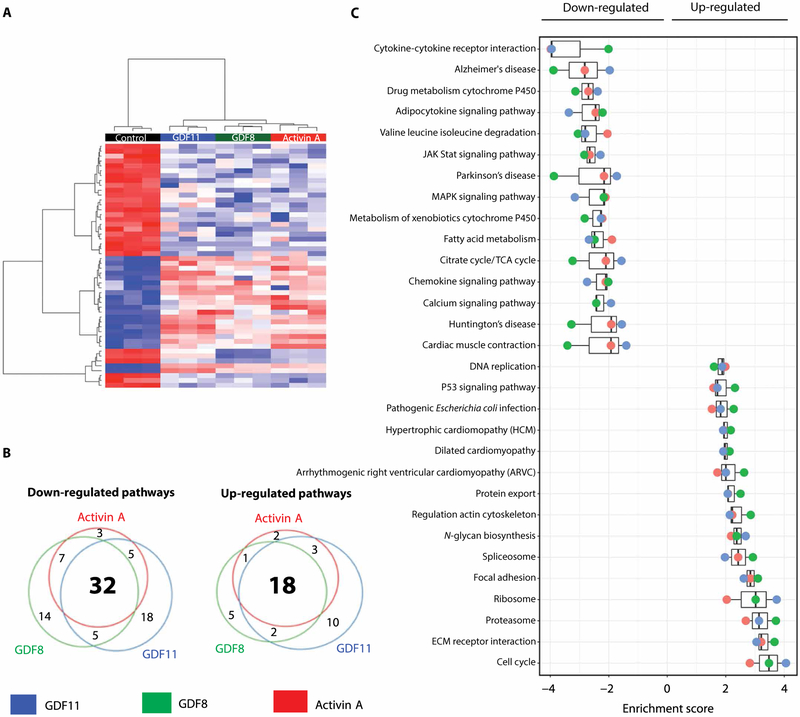
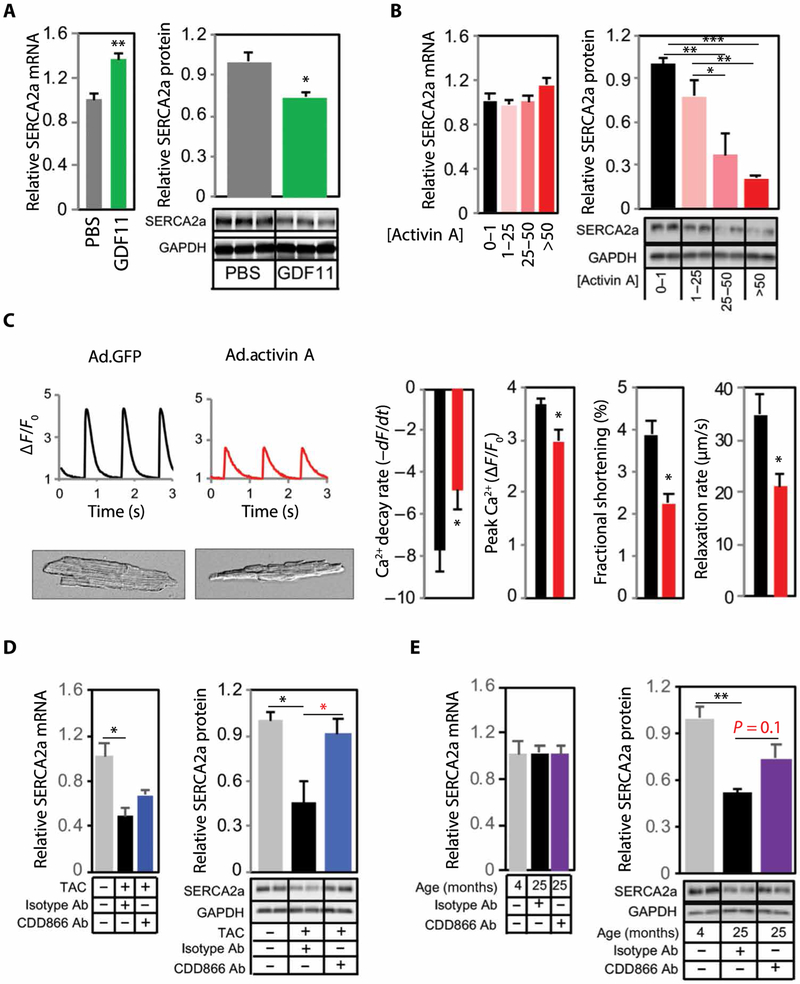
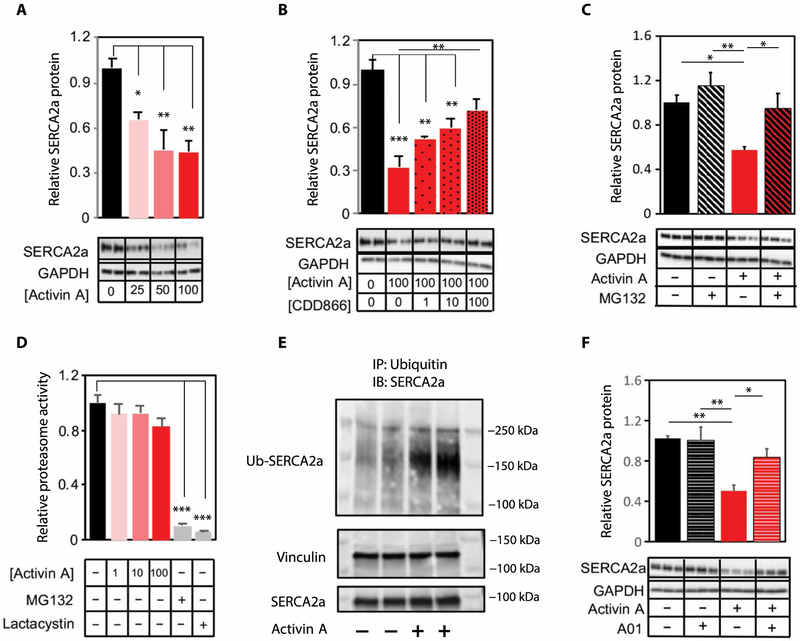
Activin type II receptor (ActRII) ligands have been implicated in muscle wasting in aging and disease. However, the role of these ligands and ActRII signaling in the heart remains unclear. Here, we investigated this catabolic pathway in human aging and heart failure (HF) using circulating follistatin-like 3 (FSTL3) as a potential indicator of systemic ActRII activity. FSTL3 is a downstream regulator of ActRII signaling, whose expression is up-regulated by the major ActRII ligands, activin A, circulating growth differentiation factor-8 (GDF8), and GDF11. In humans, we found that circulating FSTL3 increased with aging, frailty, and HF severity, correlating with an increase in circulating activins. In mice, increasing circulating activin A increased cardiac ActRII signaling and FSTL3 expression, as well as impaired cardiac function. Conversely, ActRII blockade with either clinical-stage inhibitors or genetic ablation reduced cardiac ActRII signaling while restoring or preserving cardiac function in multiple models of HF induced by aging, sarcomere mutation, or pressure overload. Using unbiased RNA sequencing, we show that activin A, GDF8, and GDF11 all induce a similar pathologic profile associated with up-regulation of the proteasome pathway in mammalian cardiomyocytes. The E3 ubiquitin ligase, Smurf1, was identified as a key downstream effector of activin-mediated ActRII signaling, which increased proteasome-dependent degradation of sarcoplasmic reticulum Ca2+ ATPase (SERCA2a), a critical determinant of cardiomyocyte function. Together, our findings suggest that increased activin/ActRII signaling links aging and HF pathobiology and that targeted inhibition of this catabolic pathway holds promise as a therapeutic strategy for multiple forms of HF.
Copyright © 2019 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
Comment in
-
ACTRII signalling implicated in HF.Nat Rev Cardiol. 2019 May;16(5):258. doi: 10.1038/s41569-019-0183-4. Nat Rev Cardiol. 2019. PMID: 30874631 No abstract available.
Similar articles
-
Activin type II receptor ligand signaling inhibition after experimental ischemic heart failure attenuates cardiac remodeling and prevents fibrosis.Am J Physiol Heart Circ Physiol. 2020 Feb 1;318(2):H378-H390. doi: 10.1152/ajpheart.00302.2019. Epub 2019 Dec 30. Am J Physiol Heart Circ Physiol. 2020. PMID: 31886717 Free PMC article.
-
Activin A and follistatin-like 3 determine the susceptibility of heart to ischemic injury.Circulation. 2009 Oct 20;120(16):1606-15. doi: 10.1161/CIRCULATIONAHA.109.872200. Epub 2009 Oct 5. Circulation. 2009. PMID: 19805648 Free PMC article.
-
ActRII or BMPR ligands inhibit skeletal myoblast differentiation, and BMPs promote heterotopic ossification in skeletal muscles in mice.Skelet Muscle. 2025 Feb 24;15(1):4. doi: 10.1186/s13395-025-00373-7. Skelet Muscle. 2025. PMID: 39994804 Free PMC article.
-
Biochemistry and Biology of GDF11 and Myostatin: Similarities, Differences, and Questions for Future Investigation.Circ Res. 2016 Apr 1;118(7):1125-41; discussion 1142. doi: 10.1161/CIRCRESAHA.116.308391. Circ Res. 2016. PMID: 27034275 Free PMC article. Review.
-
Bimagrumab: an investigational human monoclonal antibody against activin type II receptors for treating obesity.J Basic Clin Physiol Pharmacol. 2024 Oct 10;35(6):325-334. doi: 10.1515/jbcpp-2024-0065. eCollection 2024 Nov 1. J Basic Clin Physiol Pharmacol. 2024. PMID: 39385353 Review.
Cited by
-
Circulating GDF11 exacerbates myocardial injury in mice and associates with increased infarct size in humans.Cardiovasc Res. 2023 Dec 30;119(17):2729-2742. doi: 10.1093/cvr/cvad153. Cardiovasc Res. 2023. PMID: 37742057 Free PMC article.
-
Antepartum Aspirin Administration Reduces Activin A and Cardiac Global Longitudinal Strain in Preeclamptic Women.J Am Heart Assoc. 2020 Jun 16;9(12):e015997. doi: 10.1161/JAHA.119.015997. Epub 2020 Jun 4. J Am Heart Assoc. 2020. PMID: 32495688 Free PMC article.
-
Inhibition of Activin/Myostatin signalling induces skeletal muscle hypertrophy but impairs mouse testicular development.Eur J Transl Myol. 2020 Apr 1;30(1):8737. doi: 10.4081/ejtm.2019.8737. eCollection 2020 Apr 7. Eur J Transl Myol. 2020. PMID: 32499882 Free PMC article.
-
Myokines and Heart Failure: Challenging Role in Adverse Cardiac Remodeling, Myopathy, and Clinical Outcomes.Dis Markers. 2021 Jan 13;2021:6644631. doi: 10.1155/2021/6644631. eCollection 2021. Dis Markers. 2021. PMID: 33520013 Free PMC article. Review.
-
Preeclampsia: Linking Placental Ischemia with Maternal Endothelial and Vascular Dysfunction.Compr Physiol. 2020 Dec 9;11(1):1315-1349. doi: 10.1002/cphy.c200008. Compr Physiol. 2020. PMID: 33295016 Free PMC article.
References
-
- Lüscher TF, Heart failure subgroups: HFrEF, HFmrEF, and HFpEF with or without mitral regurgitation. Eur. Heart J 39, 1–4 (2018). - PubMed
-
- Shah KS, Xu H, Matsouaka RA, Bhatt DL, Heidenreich PA, Hernandez AF, Devore AD, Yancy CW, Fonarow GC, Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J. Am. Coll. Cardiol 70, 2476–2486 (2017). - PubMed
-
- Loffredo FS, Steinhauser ML, Jay SM, Gannon J, Pancoast JR, Yalamanchi P, Sinha M, Dall’Osso C, Khong D, Shadrach JL, Miller CM, Singer BS, Stewart A, Psychogios N, Gerszten RE, Hartigan AJ, Kim M-J, Serwold T, Wagers AJ, Lee RT, Growth differentiation factor 11 is a circulating factor that reverses age-related cardiac hypertrophy. Cell 153, 828–839 (2013). - PMC - PubMed
-
- Olson KA, Beatty AL, Heidecker B, Regan MC, Brody EN, Foreman T, Kato S, Mehler RE, Singer BS, Hveem K, Dalen H, Sterling DG, Lawn RM, Schiller NB, Williams SA, Whooley MA, Ganz P, Association of growth differentiation factor 11/8, putative anti-ageing factor, with cardiovascular outcomes and overall mortality in humans: Analysis of the heart and soul and HUNT3 cohorts. Eur. Heart J 36, 3426–3434 (2015). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
