

Rare Pathogenic Variants Predispose to Hepatocellular Carcinoma in Nonalcoholic Fatty Liver Disease
- PMID: 30842500
- PMCID: PMC6403344
- DOI: 10.1038/s41598-019-39998-2
Rare Pathogenic Variants Predispose to Hepatocellular Carcinoma in Nonalcoholic Fatty Liver Disease
Abstract
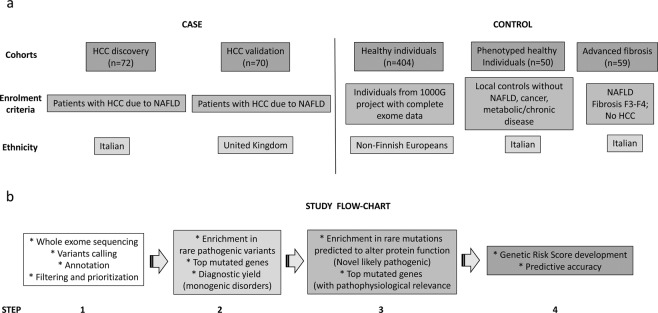
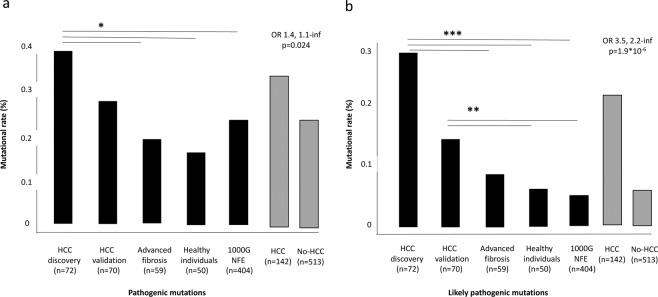
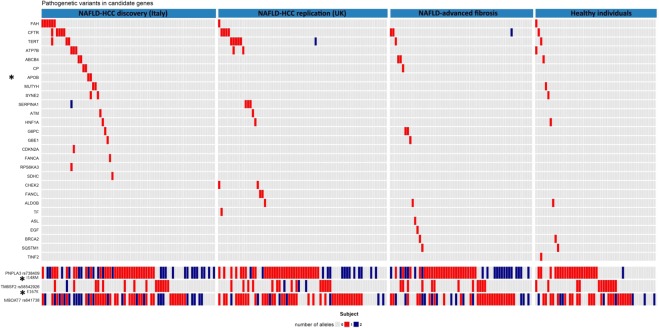
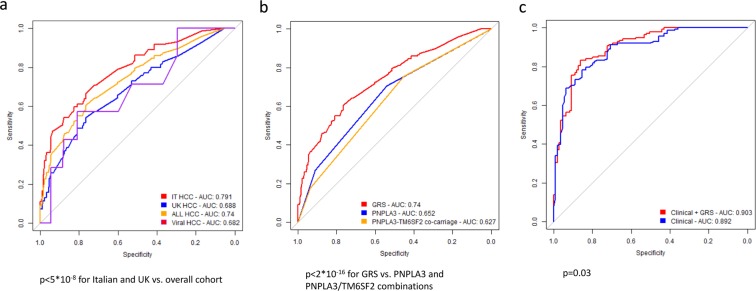
Nonalcoholic fatty liver disease (NAFLD) is a rising cause of hepatocellular carcinoma (HCC). We examined whether inherited pathogenic variants in candidate genes (n = 181) were enriched in patients with NAFLD-HCC. To this end, we resequenced peripheral blood DNA of 142 NAFLD-HCC, 59 NAFLD with advanced fibrosis, and 50 controls, and considered 404 healthy individuals from 1000 G. Pathogenic variants were defined according to ClinVar, likely pathogenic as rare variants predicted to alter protein activity. In NAFLD-HCC patients, we detected an enrichment in pathogenic (p = 0.024), and likely pathogenic variants (p = 1.9*10-6), particularly in APOB (p = 0.047). APOB variants were associated with lower circulating triglycerides and higher HDL cholesterol (p < 0.01). A genetic risk score predicted NAFLD-HCC (OR 4.96, 3.29-7.55; p = 5.1*10-16), outperforming the diagnostic accuracy of common genetic risk variants, and of clinical risk factors (p < 0.05). In conclusion, rare pathogenic variants in genes involved in liver disease and cancer predisposition are associated with NAFLD-HCC development.
Conflict of interest statement
Authors declare that they do not have any conflict of interest or competing interests relevant to the present manuscript. L.V. received speaking fees from: M.S.D. Gilead, AlfaSigma, AbbVie, participated in consulting or advisory boards for: Gilead, Pfizer, Astra Zeneca, Novo Nordisk, and received a research grant from: Gilead.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
