

Intestinal endometriosis: Diagnostic ambiguities and surgical outcomes
- PMID: 30842955
- PMCID: PMC6397811
- DOI: 10.12998/wjcc.v7.i4.441
Intestinal endometriosis: Diagnostic ambiguities and surgical outcomes
Abstract
Background: Endometriosis is a common disease for women of reproductive age. However, when it involves intestines, it is difficult to diagnose preoperatively because its symptoms overlap with other diseases and the results of evaluations can be unspecific. Thus it is important to know the clinical characteristics of intestinal endometriosis and how to exactly diagnose.
Aim: To analyze patients in whom intestinal endometriosis was diagnosed after surgical treatments, and to evaluate the clinical characteristics of preoperatively misdiagnosed cases.
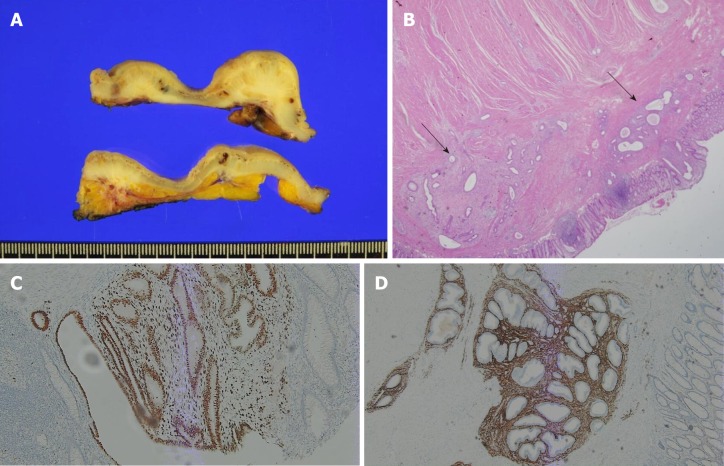
Methods: We retrospectively reviewed the pathologic reports of 30 patients diagnosed as having intestinal endometriosis based on surgical specimens between January 2000 and December 2017. We reviewed their clinical characteristics and surgical outcomes.
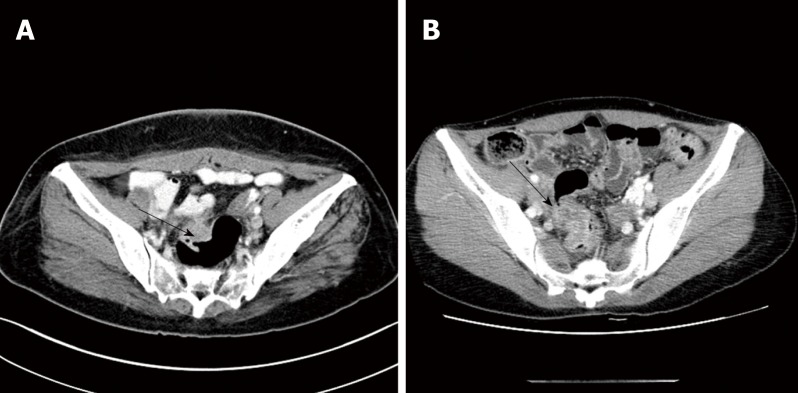
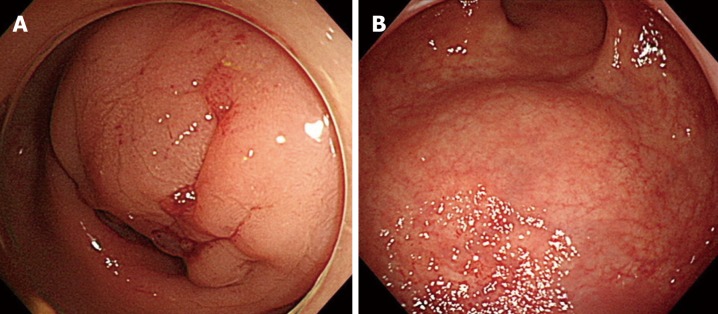
Results: Twenty-three (76.6%) patients showed symptoms associated with endometriosis, with dysmenorrhea being the most common (n = 9, 30.0%). Thirteen patients (43.3%) had a history of pelvic surgeries. Ten patients (33.3%) had a history of treatment for endometriosis. Only 4 patients (13.3%) had a diagnosis of endometriosis based on endoscopic biopsy findings. According to preoperative evaluations, 13 patients (43.3%) had an initial diagnosis of pelvic endometriosis and 17 patients (56.6%) were misdiagnosed as having other diseases. The most common misdiagnosis was submucosal tumor in the large intestine (n = 8, 26.7%), followed by malignancies of the colon/rectum (n = 3, 10.0%) and ovary (n = 3, 10.0%). According to the Clavien-Dindo classification, 5 complications were grade I or II and 2 complications were grade IIIa. The median follow-up period was 26.9 (0.6-132.1) mo, and only 1 patient had a recurrence of endometriosis.
Conclusion: Intestinal endometriosis is difficult to diagnose preoperatively because it mimics various intestinal diseases. Thus, if women of reproductive age have ambiguous symptoms and signs with nonspecific radiologic and/or endoscopic findings, intestinal endometriosis should be included in the differential diagnosis.
Keywords: Diagnosis; Endometriosis; Intestinal endometriosis; Surgery; Treatment.
Conflict of interest statement
Conflict-of-interest statement: There is no conflict of interest or no source of support.
Figures

Similar articles
-
Intestinal endometriosis treated by laparoscopic surgery: case series of 5 patients.Surg Case Rep. 2020 Mar 10;6(1):49. doi: 10.1186/s40792-020-00811-2. Surg Case Rep. 2020. PMID: 32157569 Free PMC article.
-
[Intestinal endometriosis. Three new cases and review of the literature].Ann Ital Chir. 2002 May-Jun;73(3):323-9; discussion 329-30. Ann Ital Chir. 2002. PMID: 12404901 Review. Italian.
-
Rectal Shaving Using Plasma Energy in Deep Infiltrating Endometriosis of the Rectum: Four Years of Experience.J Minim Invasive Gynecol. 2017 Nov-Dec;24(7):1121-1127. doi: 10.1016/j.jmig.2017.06.019. Epub 2017 Jun 30. J Minim Invasive Gynecol. 2017. PMID: 28673871
-
Diagnosis and management of endometriosis of the colon and rectum.Dis Colon Rectum. 1988 Dec;31(12):952-6. doi: 10.1007/BF02554893. Dis Colon Rectum. 1988. PMID: 3215101
-
[Intestinal endometriosis].Presse Med. 2012 Apr;41(4):358-66. doi: 10.1016/j.lpm.2011.07.017. Epub 2011 Oct 19. Presse Med. 2012. PMID: 22014564 Review. French.
Cited by
-
Intestinal endometriosis in a 36-year-old woman.CMAJ. 2020 Aug 17;192(33):E960. doi: 10.1503/cmaj.191471. CMAJ. 2020. PMID: 32817000 Free PMC article. No abstract available.
-
Refining MRI protocols for endometriosis: a comparative study of abbreviated and full MRI sequences.Br J Radiol. 2025 Feb 1;98(1166):287-295. doi: 10.1093/bjr/tqae230. Br J Radiol. 2025. PMID: 39531257 Free PMC article.
-
Rectosigmoid endometriosis, a rare cause of lower GI bleeding in a premenopausal woman: Case report.Int J Surg Case Rep. 2025 Aug;133:111608. doi: 10.1016/j.ijscr.2025.111608. Epub 2025 Jul 4. Int J Surg Case Rep. 2025. PMID: 40618668 Free PMC article.
-
Endometriosis with colonic and rectal involvement: surgical approach and outcomes in 142 patients.Langenbecks Arch Surg. 2023 Sep 29;408(1):385. doi: 10.1007/s00423-023-03095-w. Langenbecks Arch Surg. 2023. PMID: 37773225
-
Gastrointestinal function outcomes following radical and conservative colorectal surgery for deep endometriosis: A systematic review and meta-analysis.Acta Obstet Gynecol Scand. 2025 Apr;104(4):615-628. doi: 10.1111/aogs.15023. Epub 2025 Feb 17. Acta Obstet Gynecol Scand. 2025. PMID: 39962770 Free PMC article.
References
-
- Remorgida V, Ferrero S, Fulcheri E, Ragni N, Martin DC. Bowel endometriosis: presentation, diagnosis, and treatment. Obstet Gynecol Surv. 2007;62:461–470. - PubMed
-
- Campagnacci R, Perretta S, Guerrieri M, Paganini AM, De Sanctis A, Ciavattini A, Lezoche E. Laparoscopic colorectal resection for endometriosis. Surg Endosc. 2005;19:662–664. - PubMed
-
- Meuleman C, Tomassetti C, D'Hoore A, Van Cleynenbreugel B, Penninckx F, Vergote I, D'Hooghe T. Surgical treatment of deeply infiltrating endometriosis with colorectal involvement. Hum Reprod Update. 2011;17:311–326. - PubMed
LinkOut - more resources
Full Text Sources
