

Long-term Somatic Disease Risk in Adult Danish Cancer Survivors
- PMID: 30844031
- PMCID: PMC6459216
- DOI: 10.1001/jamaoncol.2018.7192
Long-term Somatic Disease Risk in Adult Danish Cancer Survivors
Erratum in
-
Affiliation Added.JAMA Oncol. 2019 Apr 1;5(4):579. doi: 10.1001/jamaoncol.2019.0705. JAMA Oncol. 2019. PMID: 30973604 Free PMC article. No abstract available.
Abstract
Importance: Long-term health effects of cancer in adult survivors are a major concern; however, it is difficult to differentiate between the consequences of cancer and cancer treatment and those of normal aging or comorbidity.
Objectives: To provide an overview and investigate the temporal pattern of hospitalizations for medically verified incident somatic disease in adult survivors compared with cancer-free comparison people, taking into consideration pretreatment comorbidity and the socioeconomic position of the participants.
Design, setting, and participants: In this nationwide, population-based cohort-cohort study, 458 646 survivors of the 12 most frequent first primary cancers listed in the Danish Cancer Registry between January 1, 1997, and December 31, 2014, and 2 121 567 matched cancer-free comparison people were identified from the Danish Central Population Registry. Hospitalizations for somatic diseases after cancer diagnosis or study entry were identified from the National Patient Register and stratified according to the 11 main diagnostic groups in the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision. A cohort of cancer survivors was formed for each combination of cancer type and diagnostic group, with a corresponding group of cancer-free people, resulting in 132 unique cohorts. Data analysis was performed from September 1, 2017, to January 15, 2018.
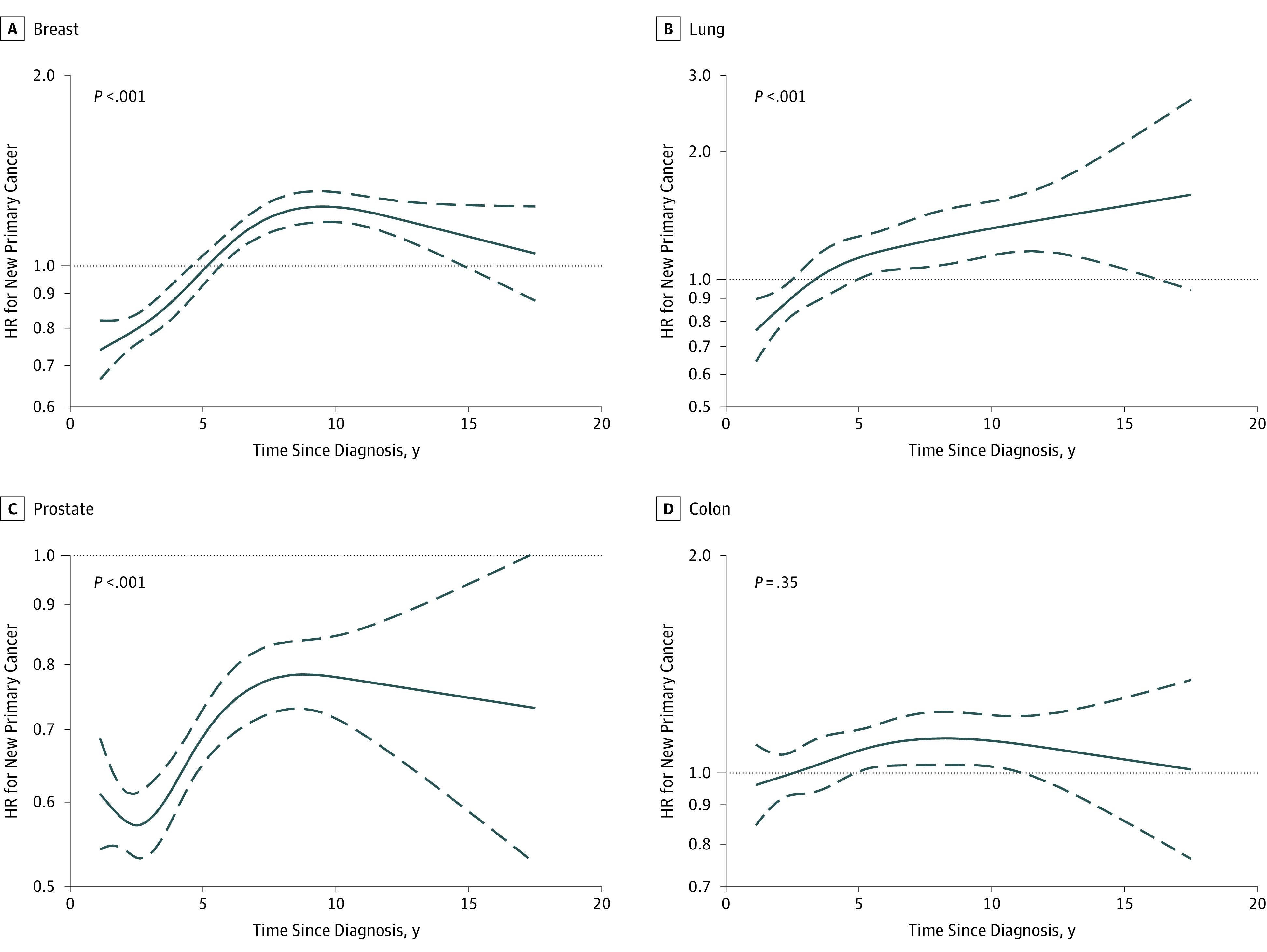
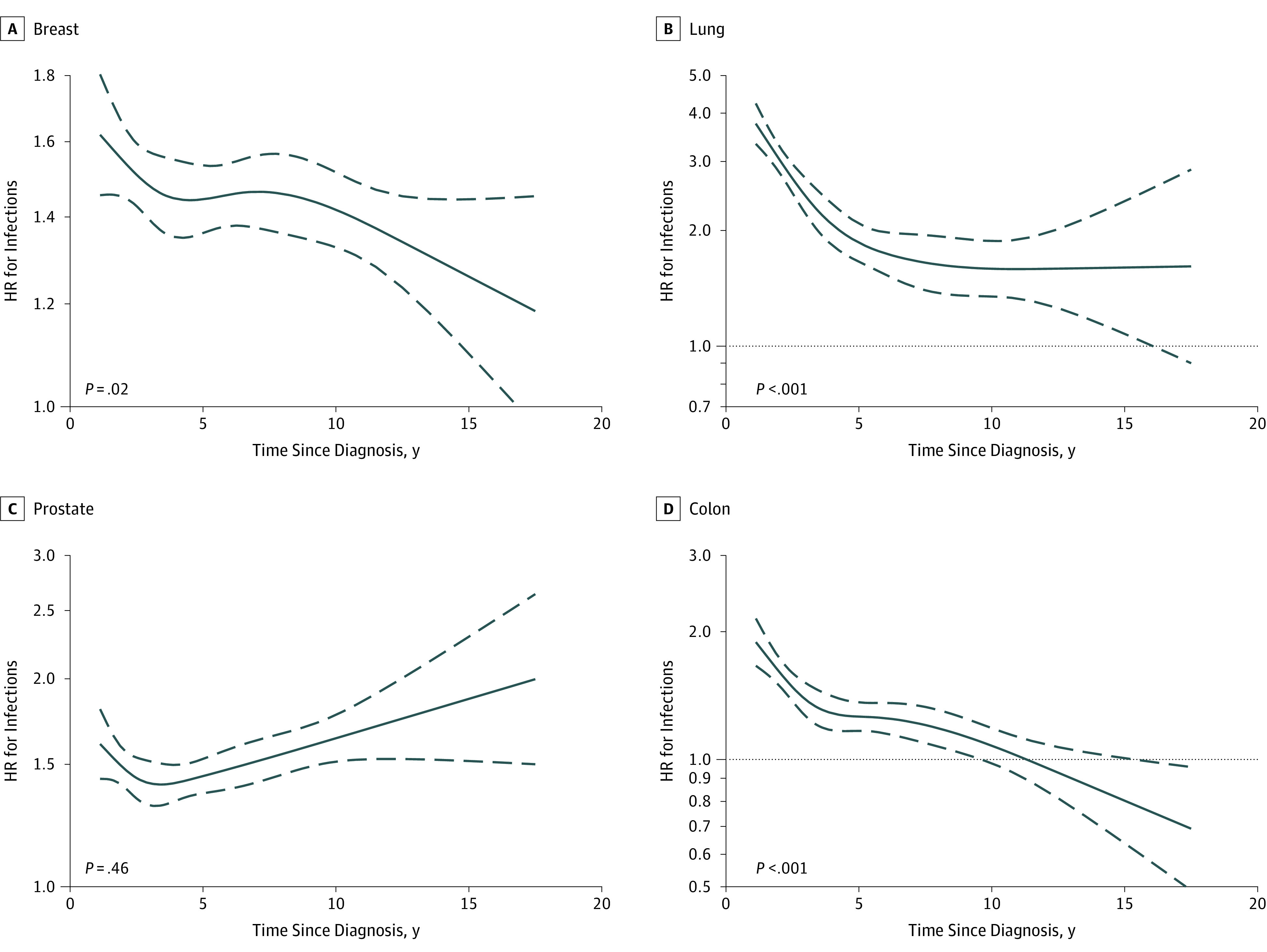
Main outcomes and measures: Risk of hospitalization and the temporal pattern of incidence were analyzed in Cox proportional hazards regression models. Cumulative incidence proportions were calculated by the pseudo-observation method.
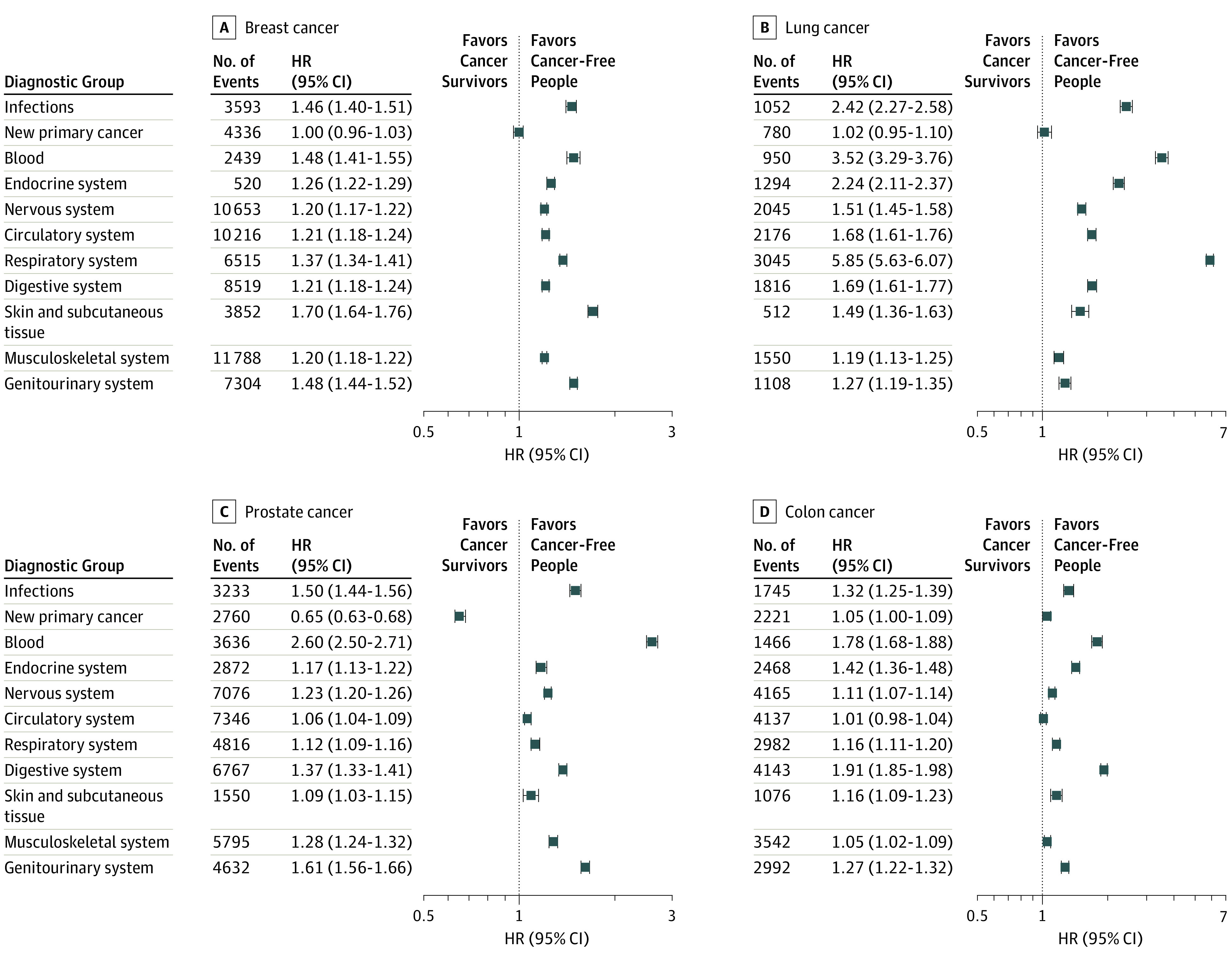
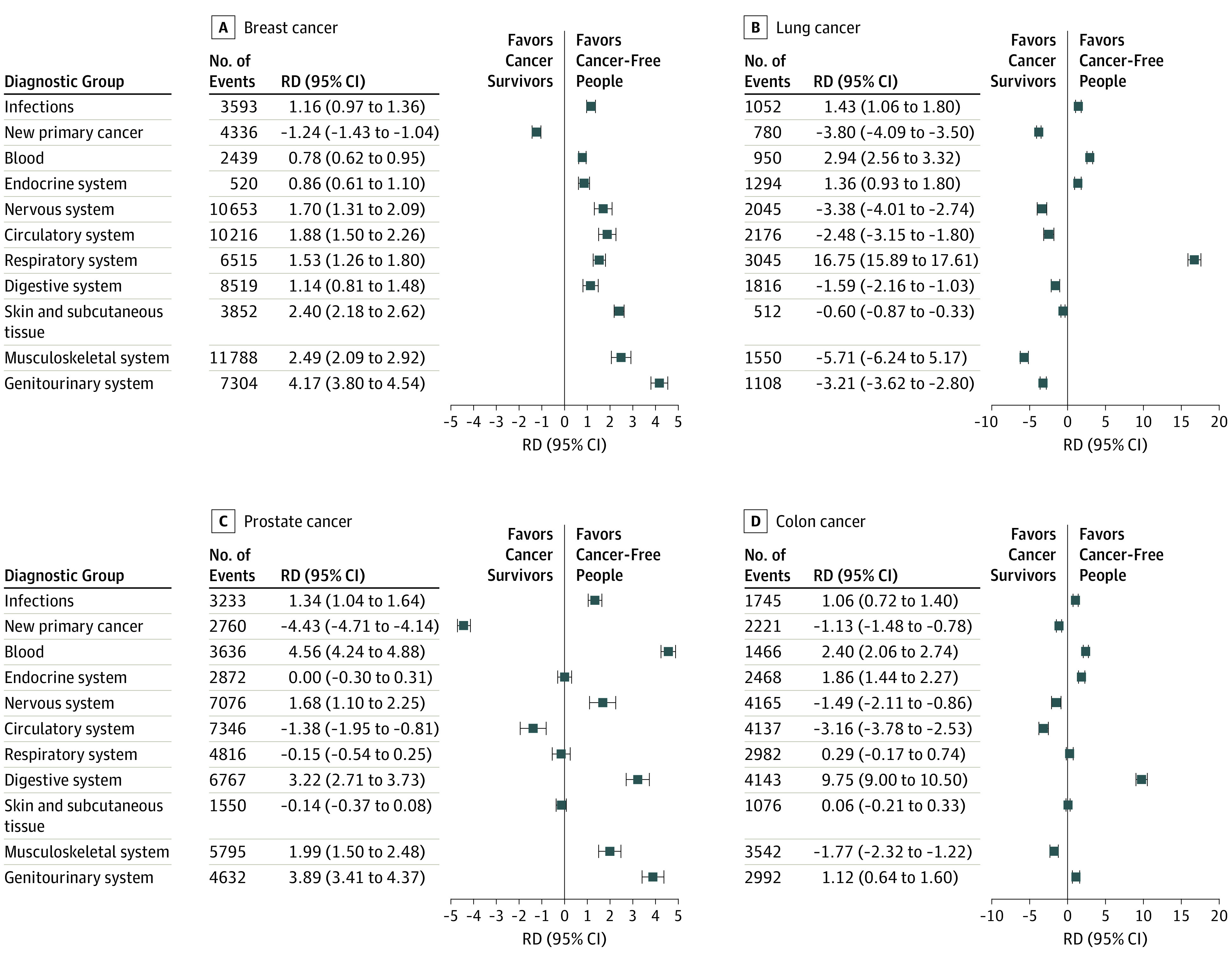
Results: A total of 2 580 213 people were investigated, of whom 458 646 were cancer survivors (mean [SD] age, 69 [11.6] years; 230 793 [50.3%] male and 227 853 [49.7%] female) and 2 121 567 were comparison people (mean [SD] age, 69 [11.5] years; 1 054 465 [49.7%] male and 1 067 102 [50.3%] female). More cancer survivors vs comparison people had comorbid conditions at the time of cancer diagnosis or study entry (Charlson Comorbidity Index ≥1: 19% vs 13%). Overall, the risk of hospitalizations for somatic diseases was significantly higher for cancer survivors in almost all diagnostic groups (eg, diseases in the nervous system among breast cancer survivors: hazard ratio, 1.20; 95% CI, 1.17-1.22; diseases in the respiratory system in lung cancer survivors: hazard ratio, 5.85; 95% CI, 5.63-6.07; and diseases in blood and blood-forming organs in prostate cancer survivors: hazard ratio, 2.60; 95% CI, 2.50-2.71).
Conclusions and relevance: The findings suggest that adult survivors of the 12 most common cancers are at significantly higher risk for a broad range of somatic diseases that require hospitalization compared with matched cancer-free comparison people. The results of this study suggest the importance of close, targeted monitoring for new somatic disease during follow-up care of cancer survivors.
Conflict of interest statement
Figures
Comment in
-
Health burden in cancer survivors: below the tip of the iceberg.Nat Rev Clin Oncol. 2019 Aug;16(8):467-468. doi: 10.1038/s41571-019-0226-0. Nat Rev Clin Oncol. 2019. PMID: 31101878 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
