

Composite Pain Biomarker Signatures for Objective Assessment and Effective Treatment
- PMID: 30844399
- PMCID: PMC6800055
- DOI: 10.1016/j.neuron.2019.02.019
Composite Pain Biomarker Signatures for Objective Assessment and Effective Treatment
Abstract
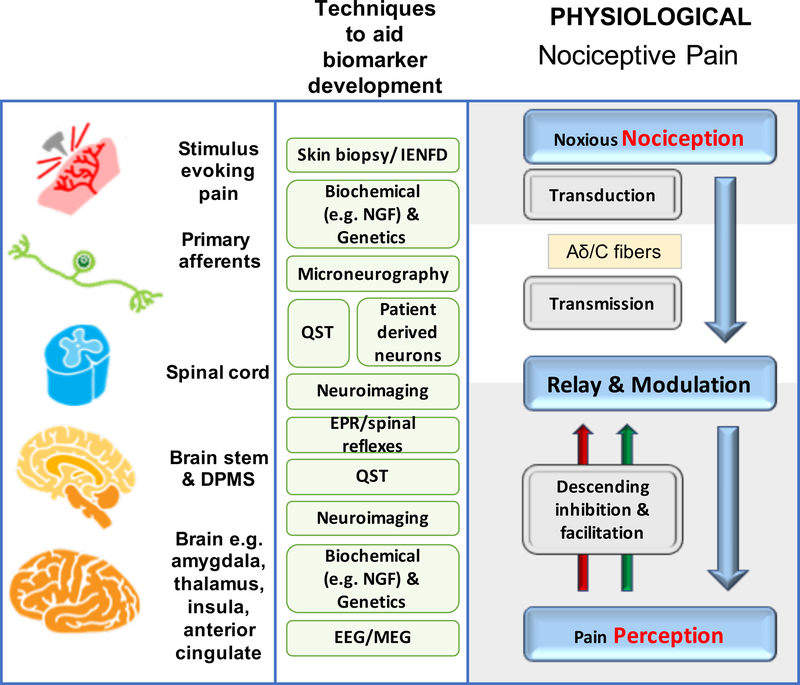
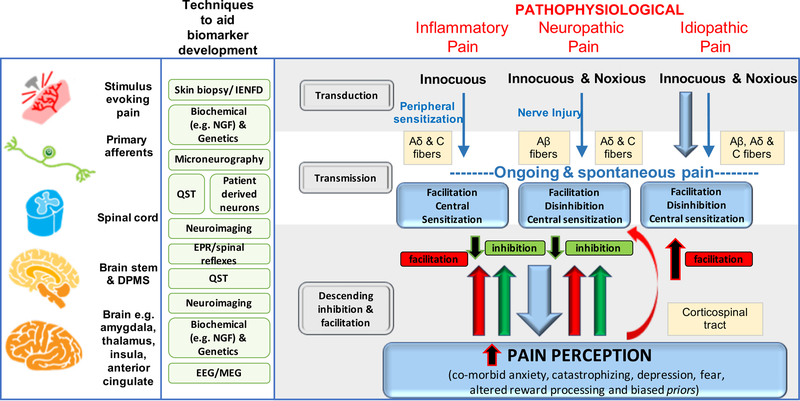
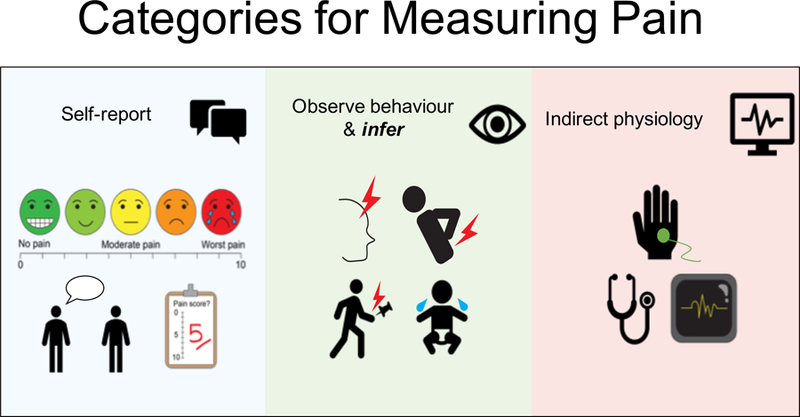
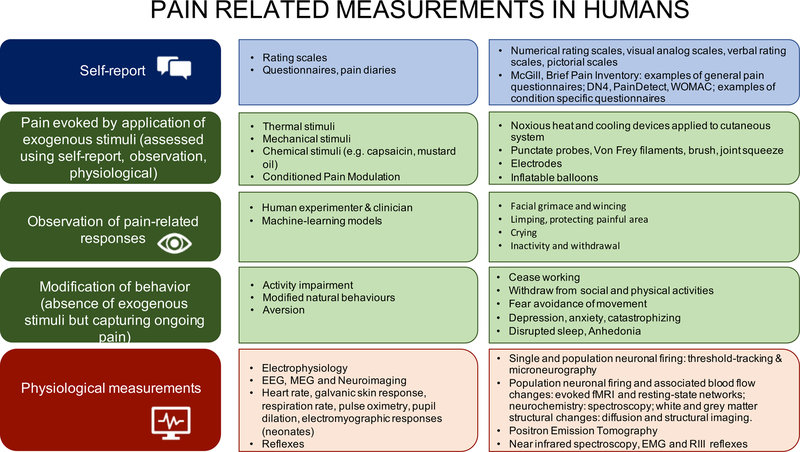
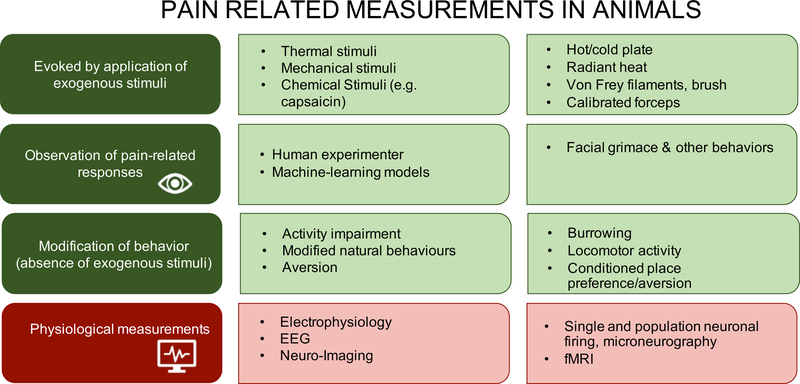
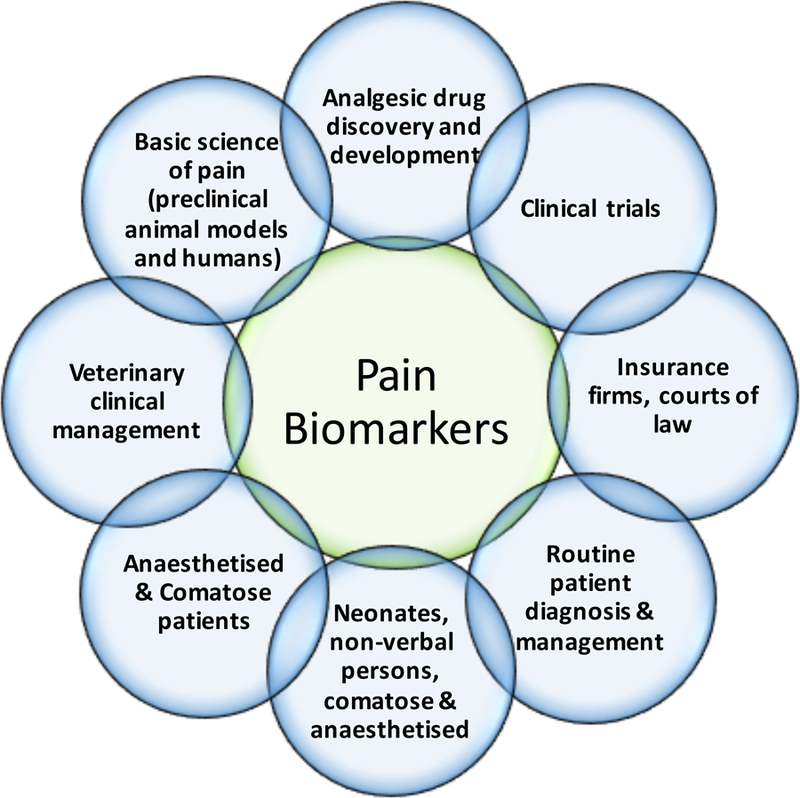
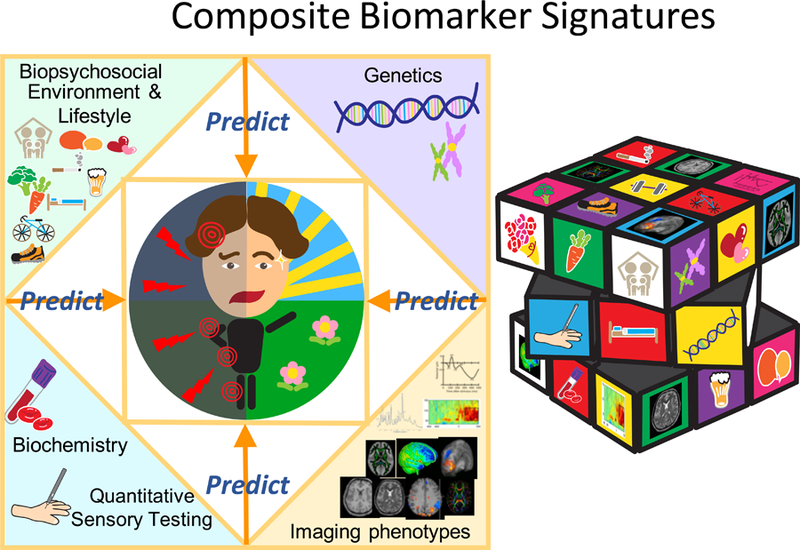
Pain is a subjective sensory experience that can, mostly, be reported but cannot be directly measured or quantified. Nevertheless, a suite of biomarkers related to mechanisms, neural activity, and susceptibility offer the possibility-especially when used in combination-to produce objective pain-related indicators with the specificity and sensitivity required for diagnosis and for evaluation of risk of developing pain and of analgesic efficacy. Such composite biomarkers will also provide improved understanding of pain pathophysiology.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests:
Clifford Woolf is on SAB of Biogen and is a founder of Nocion Therapeutics.
Nick Andrews has founding shares in Nocion Therapeutics.
Irene Tracey is on the Neuroscience SAB of Amgen and is part of Innovative Medicines Initiative PainCare-Biopain. She has a patent on depth of anaesthesia monitoring.
Figures
References
-
- Alloza C, Cox SR, Blesa Cabez M, Redmond P, Whalley HC, Ritchie SJ, Munoz Maniega S, Valdes Hernandez MDC, Tucker-Drob EM, Lawrie SM, et al. (2018). Polygenic risk score for schizophrenia and structural brain connectivity in older age: A longitudinal connectome and tractography study. Neuroimage 183, 884–896. - PMC - PubMed
-
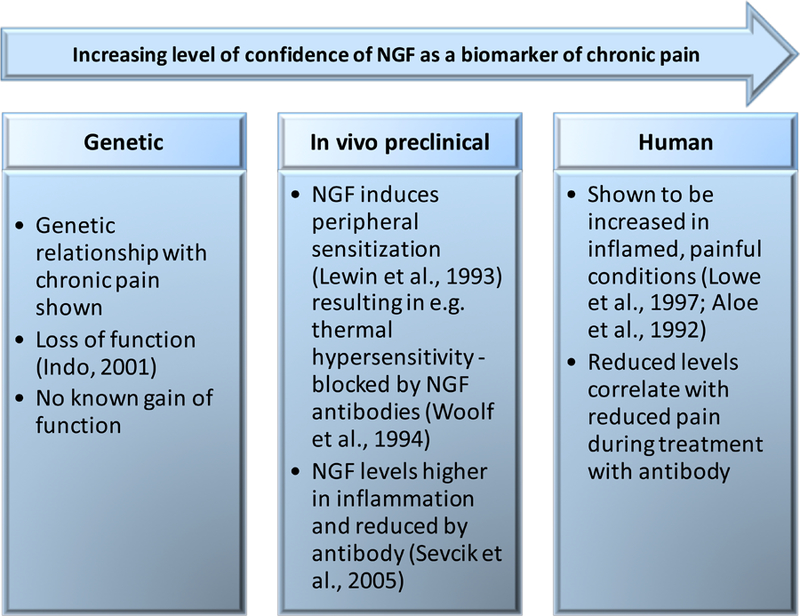
- Aloe L, Tuveri MA, Carcassi U, and Levi-Montalcini R (1992). Nerve growth factor in the synovial fluid of patients with chronic arthritis. Arthritis Rheum 35, 351–355. - PubMed
-
- Andrews N, Legg E, Lisak D, Issop Y, Richardson D, Harper S, Pheby T, Huang W, Burgess G, Machin I, and Rice AS. (2012). Spontaneous burrowing behaviour in the rat is reduced by peripheral nerve injury or inflammation associated pain. Eur J Pain 16, 485–495. - PubMed
-
- Angeby Moller K, Svard H, Suominen A, Immonen J, Holappa J, and Stenfors C. (2018). Gait analysis and weight bearing in pre-clinical joint pain research. J Neurosci Methods 300, 92–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
