

Titration of Medical Therapy for Heart Failure With Reduced Ejection Fraction
- PMID: 30844480
- PMCID: PMC7197490
- DOI: 10.1016/j.jacc.2019.02.015
Titration of Medical Therapy for Heart Failure With Reduced Ejection Fraction
Abstract
Background: Guidelines recommend that patients with heart failure with reduced ejection fraction (HFrEF) have medical therapy titrated to target doses derived from clinical trials, as tolerated. The degree to which titration occurs in contemporary U.S. practice is unknown.
Objectives: This study sought to characterize longitudinal titration of HFrEF medical therapy in clinical practice and to identify associated factors and reasons for medication changes.
Methods: Among 2,588 U.S. outpatients with chronic HFrEF in the CHAMP-HF (Change the Management of Patients with Heart Failure) registry with complete medication data and no contraindications to medical therapy, use and dose of angiotensin-converting enzyme inhibitor (ACEI)/angiotensin II receptor blocker (ARB), angiotensin receptor-neprilysin inhibitor (ARNI), beta-blocker, and mineralocorticoid receptor antagonist (MRA) were examined at baseline and at 12-month follow-up.
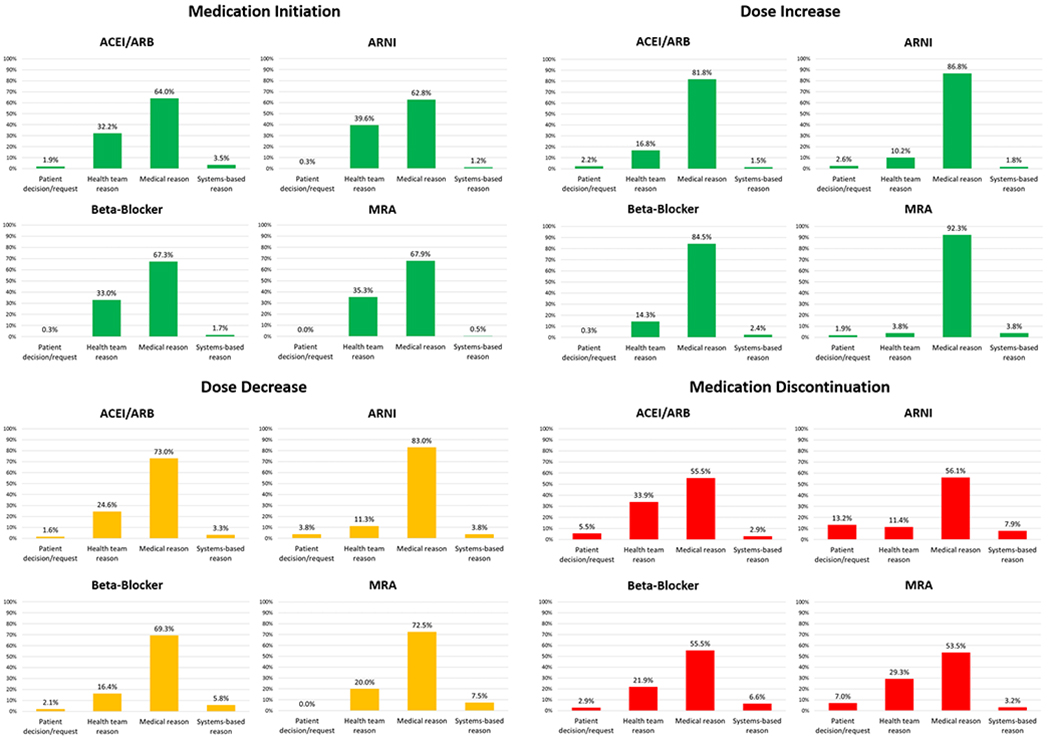
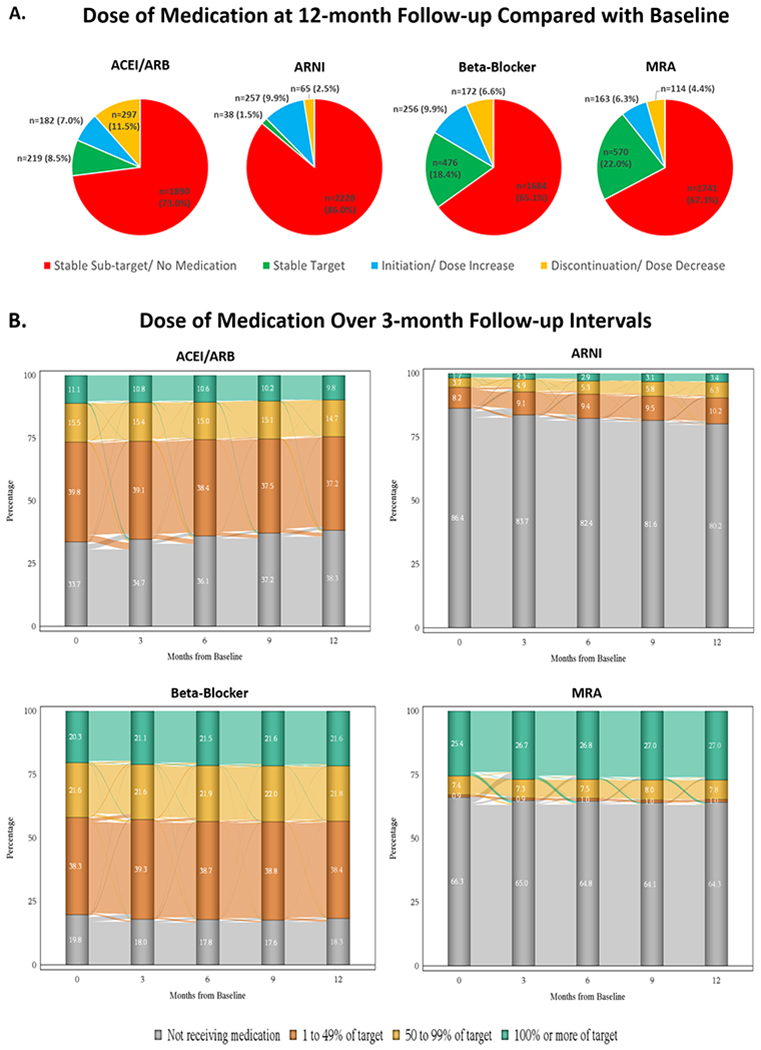
Results: At baseline, 658 (25%), 525 (20%), 287 (11%), and 45 (2%) patients were receiving target doses of MRA, beta-blocker, ACEI/ARB, and ARNI therapy, respectively. At 12 months, proportions of patients with medication initiation or dose increase were 6% for MRA, 10% for beta-blocker, 7% for ACEI/ARB, and 10% for ARNI; corresponding proportions with discontinuation or dose decrease were 4%, 7%, 11%, and 3%, respectively. Over 12 months, <1% of patients were simultaneously treated with target doses of ACEI/ARB/ARNI, beta-blocker, and MRA. In multivariate analysis, across the classes of medications, multiple patient characteristics were associated with a higher likelihood of initiation or dose increase (e.g., previous HF hospitalization, higher blood pressure, lower ejection fraction) and discontinuation or dose decrease (e.g., previous HF hospitalization, impaired quality of life, more severe functional class). Medical reasons were the most common reasons for discontinuations and dose decreases of each therapy, but the relative contributions from patient preference, health team, and systems-based reasons varied by medication.
Conclusions: In this contemporary U.S. registry, most eligible HFrEF patients did not receive target doses of medical therapy at any point during follow-up, and few patients had doses increased over time. Although most patients had no alterations in medical therapy, multiple clinical factors were independently associated with medication changes. Further quality improvement efforts are urgently needed to improve guideline-directed medication titration for HFrEF.
Keywords: dose; heart failure; medication; reduced ejection fraction; registry.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Reasons for Lack of Improvement in Treatment With Evidence-Based Therapies in Heart Failure.J Am Coll Cardiol. 2019 May 21;73(19):2384-2387. doi: 10.1016/j.jacc.2019.03.464. J Am Coll Cardiol. 2019. PMID: 31097156 No abstract available.
-
Machine Learning Could Facilitate Optimal Titration of Guideline-Directed Medical Therapy in Heart Failure.J Am Coll Cardiol. 2019 Sep 10;74(10):1424-1425. doi: 10.1016/j.jacc.2019.06.063. J Am Coll Cardiol. 2019. PMID: 31488282 No abstract available.
-
Clinically Optimal Versus "Target" Doses in Heart Failure.J Am Coll Cardiol. 2019 Sep 10;74(10):1425. doi: 10.1016/j.jacc.2019.06.062. J Am Coll Cardiol. 2019. PMID: 31488283 No abstract available.
References
-
- Yancy CW, Jessup M, Bozkurt B et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;62:e147–239. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol 2017;70:776–803. - PubMed
-
- Yancy CW, Januzzi JL, Jr., Allen LA et al. 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol 2018;71:201–230. - PubMed
-
- Greene SJ, Butler J, Albert NM et al. Medical Therapy for Heart Failure With Reduced Ejection Fraction: The CHAMP-HF Registry. J Am Coll Cardiol 2018;72:351–366. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
