

Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint
- PMID: 30845034
- PMCID: PMC6467578
- DOI: 10.2106/JBJS.18.00022
Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint
Abstract
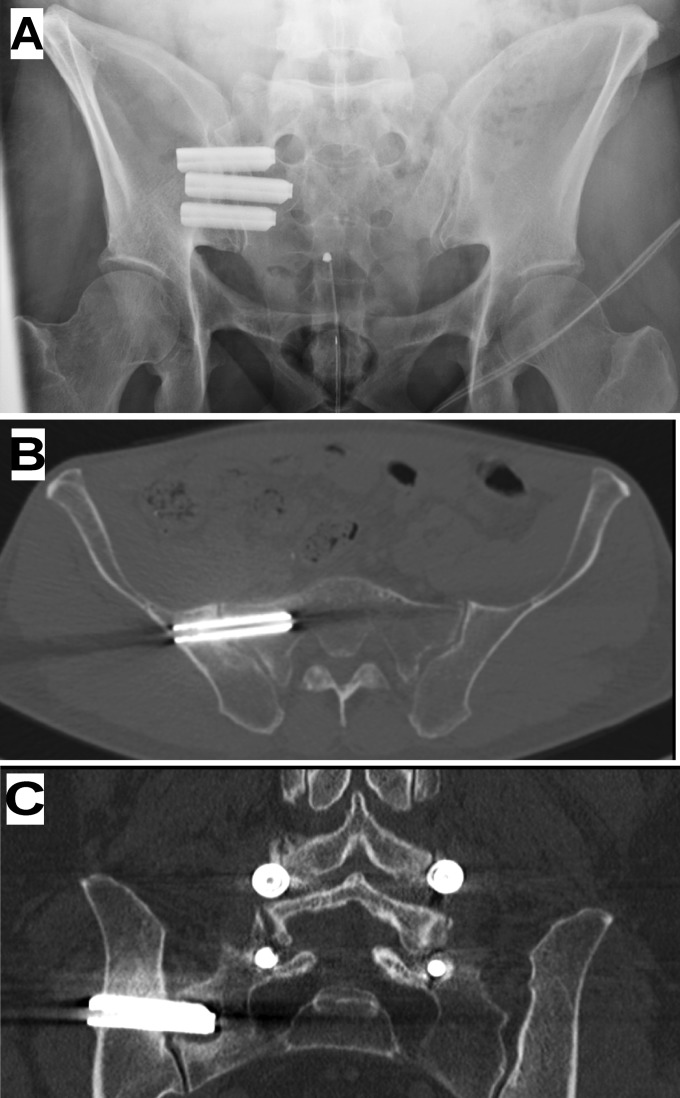
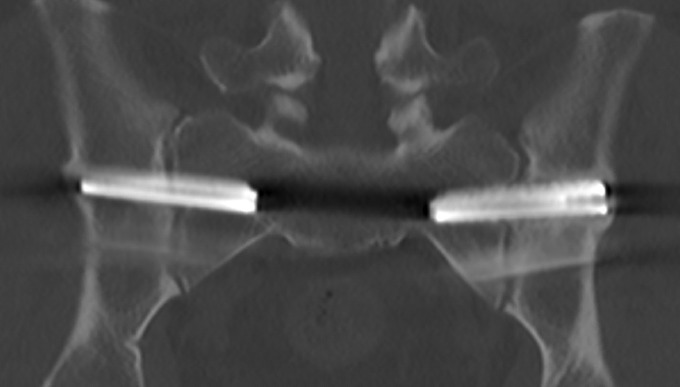
Background: Sacroiliac joint pain is increasingly recognized as a cause of low back pain. We compared the safety and effectiveness of minimally invasive sacroiliac joint arthrodesis using triangular titanium implants and conservative management in patients with chronic sacroiliac joint pain.
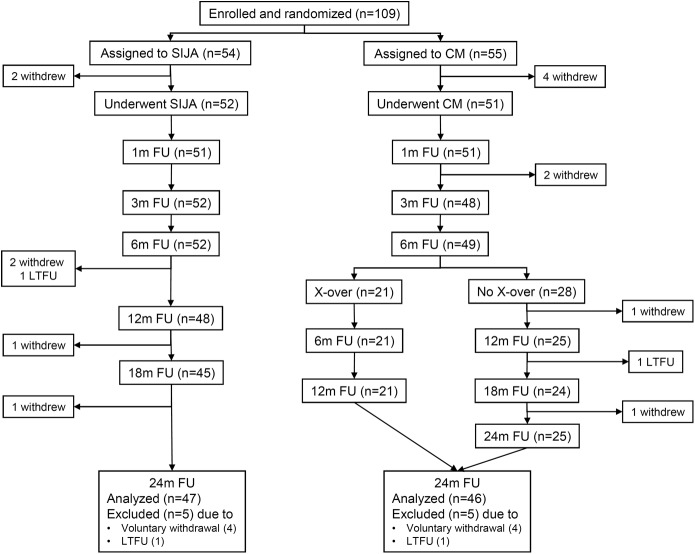
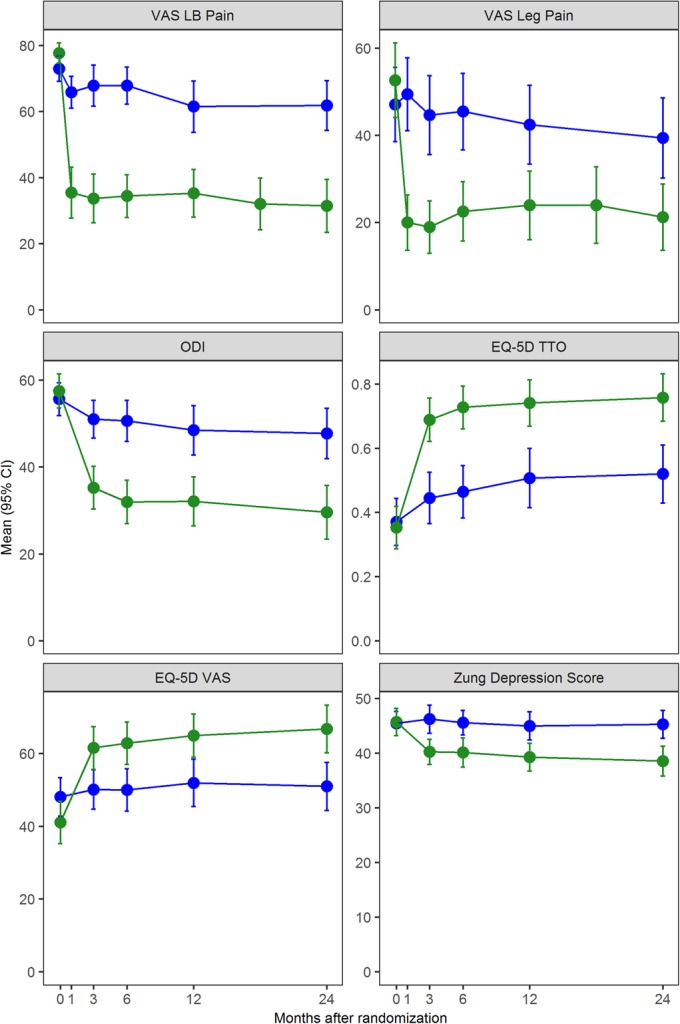
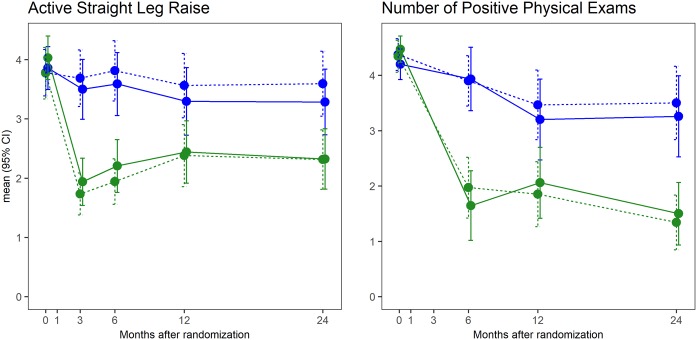
Methods: This study was a prospective, multicenter randomized controlled trial of adults with chronic sacroiliac joint pain assigned to either conservative management or sacroiliac joint arthrodesis with triangular titanium implants. The study end points included self-rated low back pain (visual analog scale [VAS]), back dysfunction (Oswestry Disability Index [ODI]), and quality of life. Ninety percent of subjects in both groups completed the study.
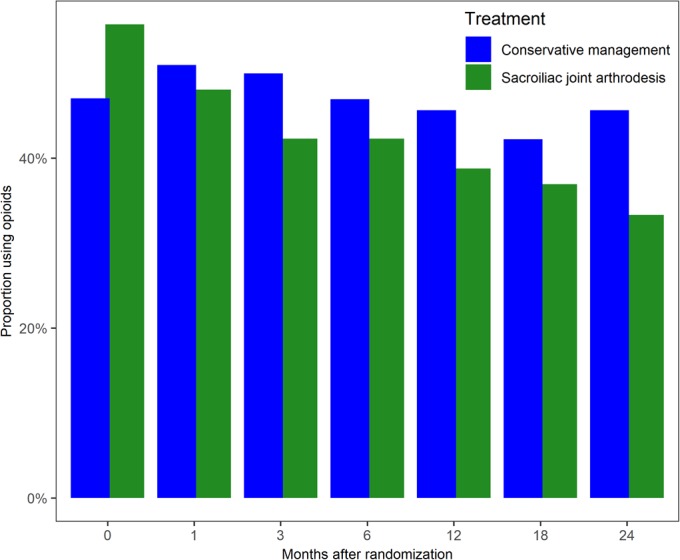
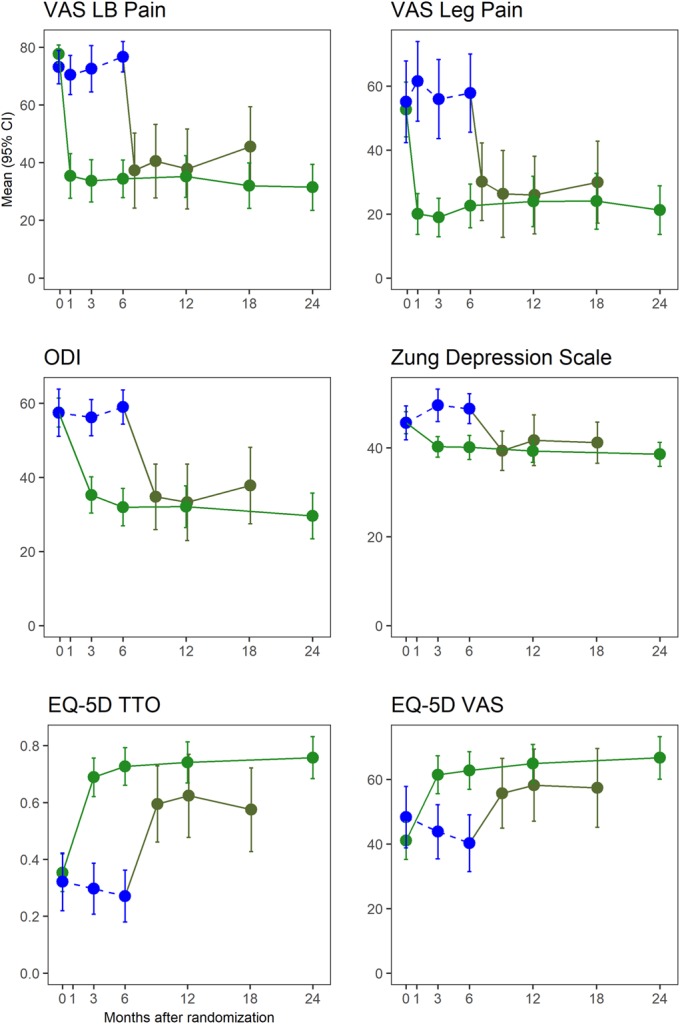
Results: Between June 6, 2013, and May 15, 2015, 103 subjects were randomly assigned to conservative management (n = 51) or sacroiliac joint arthrodesis (n = 52). At 2 years, the mean low back pain improved by 45 points (95% confidence interval [CI], 37 to 54 points) after sacroiliac joint arthrodesis and 11 points (95% CI, 2 to 20 points) after conservative management, with a mean difference between groups of 34 points (p < 0.0001). The mean ODI improved by 26 points (95% CI, 21 to 32 points) after sacroiliac joint arthrodesis and 8 points (95% CI, 2 to 14 points) after conservative management, with a mean difference between groups of 18 points (p < 0.0001). Parallel improvements were seen in quality of life. In the sacroiliac joint arthrodesis group, the prevalence of opioid use decreased from 56% at baseline to 33% at 2 years (p = 0.009), and no significant change was observed in the conservative management group (47.1% at baseline and 45.7% at 2 years). Subjects in the conservative management group, after crossover to the surgical procedure, showed improvements in all measures similar to those originally assigned to sacroiliac joint arthrodesis. In the first 6 months, the frequency of adverse events did not differ between groups (p = 0.664). By month 24, we observed 39 severe adverse events after sacroiliac joint arthrodesis, including 2 cases of sacroiliac joint pain, 1 case of a postoperative gluteal hematoma, and 1 case of postoperative nerve impingement. The analysis of computed tomographic (CT) imaging at 12 months after sacroiliac joint arthrodesis showed radiolucencies adjacent to 8 implants (4.0% of all implants).
Conclusions: For patients with chronic sacroiliac joint pain due to joint degeneration or disruption, minimally invasive sacroiliac joint arthrodesis with triangular titanium implants was safe and more effective throughout 2 years in improving pain, disability, and quality of life compared with conservative management.
Level of evidence: Therapeutic Level I. See Instructions for Authors for a complete description of levels of evidence.
Figures
Comment in
-
The Opaque Sacroiliac Joint: Commentary on an article by Julius Dengler, MD, et al.: "Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint".J Bone Joint Surg Am. 2019 Mar 6;101(5):e19. doi: 10.2106/JBJS.18.01254. J Bone Joint Surg Am. 2019. PMID: 30845045 No abstract available.
-
Is minimally invasive sacroiliac joint arthrodesis the treatment of choice for sacroiliac joint dysfunction?J Spine Surg. 2019 Sep;5(3):378-380. doi: 10.21037/jss.2019.06.01. J Spine Surg. 2019. PMID: 31663050 Free PMC article. No abstract available.
-
Minimally invasive sacroiliac joint fusion vs. conservative management for chronic sacroiliac joint pain.J Spine Surg. 2019 Sep;5(3):381-383. doi: 10.21037/jss.2019.06.10. J Spine Surg. 2019. PMID: 31663051 Free PMC article. No abstract available.
-
Sacroiliac joint pain: is the medical world aware enough of its existence? Why not considering sacroiliac joint fusion in the recalcitrant cases?J Spine Surg. 2019 Sep;5(3):384-386. doi: 10.21037/jss.2019.06.11. J Spine Surg. 2019. PMID: 31663052 Free PMC article. No abstract available.
References
-
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basáñez MG, Baxter A, Bell ML, Benjamin EJ, Bennett D, Bernabé E, Bhalla K, Bhandari B, Bikbov B, Bin Abdulhak A, Birbeck G, Black JA, Blencowe H, Blore JD, Blyth F, Bolliger I, Bonaventure A, Boufous S, Bourne R, Boussinesq M, Braithwaite T, Brayne C, Bridgett L, Brooker S, Brooks P, Brugha TS, Bryan-Hancock C, Bucello C, Buchbinder R, Buckle G, Budke CM, Burch M, Burney P, Burstein R, Calabria B, Campbell B, Canter CE, Carabin H, Carapetis J, Carmona L, Cella C, Charlson F, Chen H, Cheng AT, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahiya M, Dahodwala N, Damsere-Derry J, Danaei G, Davis A, De Leo D, Degenhardt L, Dellavalle R, Delossantos A, Denenberg J, Derrett S, Des Jarlais DC, Dharmaratne SD, Dherani M, Diaz-Torne C, Dolk H, Dorsey ER, Driscoll T, Duber H, Ebel B, Edmond K, Elbaz A, Ali SE, Erskine H, Erwin PJ, Espindola P, Ewoigbokhan SE, Farzadfar F, Feigin V, Felson DT, Ferrari A, Ferri CP, Fèvre EM, Finucane MM, Flaxman S, Flood L, Foreman K, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabbe BJ, Gabriel SE, Gakidou E, Ganatra HA, Garcia B, Gaspari F, Gillum RF, Gmel G, Gosselin R, Grainger R, Groeger J, Guillemin F, Gunnell D, Gupta R, Haagsma J, Hagan H, Halasa YA, Hall W, Haring D, Haro JM, Harrison JE, Havmoeller R, Hay RJ, Higashi H, Hill C, Hoen B, Hoffman H, Hotez PJ, Hoy D, Huang JJ, Ibeanusi SE, Jacobsen KH, James SL, Jarvis D, Jasrasaria R, Jayaraman S, Johns N, Jonas JB, Karthikeyan G, Kassebaum N, Kawakami N, Keren A, Khoo JP, King CH, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lalloo R, Laslett LL, Lathlean T, Leasher JL, Lee YY, Leigh J, Lim SS, Limb E, Lin JK, Lipnick M, Lipshultz SE, Liu W, Loane M, Ohno SL, Lyons R, Ma J, Mabweijano J, MacIntyre MF, Malekzadeh R, Mallinger L, Manivannan S, Marcenes W, March L, Margolis DJ, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGill N, McGrath J, Medina-Mora ME, Meltzer M, Mensah GA, Merriman TR, Meyer AC, Miglioli V, Miller M, Miller TR, Mitchell PB, Mocumbi AO, Moffitt TE, Mokdad AA, Monasta L, Montico M, Moradi-Lakeh M, Moran A, Morawska L, Mori R, Murdoch ME, Mwaniki MK, Naidoo K, Nair MN, Naldi L, Narayan KM, Nelson PK, Nelson RG, Nevitt MC, Newton CR, Nolte S, Norman P, Norman R, O’Donnell M, O’Hanlon S, Olives C, Omer SB, Ortblad K, Osborne R, Ozgediz D, Page A, Pahari B, Pandian JD, Rivero AP, Patten SB, Pearce N, Padilla RP, Perez-Ruiz F, Perico N, Pesudovs K, Phillips D, Phillips MR, Pierce K, Pion S, Polanczyk GV, Polinder S, Pope CA, 3rd, Popova S, Porrini E, Pourmalek F, Prince M, Pullan RL, Ramaiah KD, Ranganathan D, Razavi H, Regan M, Rehm JT, Rein DB, Remuzzi G, Richardson K, Rivara FP, Roberts T, Robinson C, De Leòn FR, Ronfani L, Room R, Rosenfeld LC, Rushton L, Sacco RL, Saha S, Sampson U, Sanchez-Riera L, Sanman E, Schwebel DC, Scott JG, Segui-Gomez M, Shahraz S, Shepard DS, Shin H, Shivakoti R, Singh D, Singh GM, Singh JA, Singleton J, Sleet DA, Sliwa K, Smith E, Smith JL, Stapelberg NJ, Steer A, Steiner T, Stolk WA, Stovner LJ, Sudfeld C, Syed S, Tamburlini G, Tavakkoli M, Taylor HR, Taylor JA, Taylor WJ, Thomas B, Thomson WM, Thurston GD, Tleyjeh IM, Tonelli M, Towbin JA, Truelsen T, Tsilimbaris MK, Ubeda C, Undurraga EA, van der Werf MJ, van Os J, Vavilala MS, Venketasubramanian N, Wang M, Wang W, Watt K, Weatherall DJ, Weinstock MA, Weintraub R, Weisskopf MG, Weissman MM, White RA, Whiteford H, Wiersma ST, Wilkinson JD, Williams HC, Williams SR, Witt E, Wolfe F, Woolf AD, Wulf S, Yeh PH, Zaidi AK, Zheng ZJ, Zonies D, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012. December 15;380(9859):2163-96. - PMC - PubMed
-
- Volkow ND. America’s addiction to opioids: heroin and prescription drug abuse. 2014. May 14 https://www.drugabuse.gov/about-nida/legislative-activities/testimony-to.... Accessed 2018 Oct 15.
-
- Bernard TN, Jr, Kirkaldy-Willis WH. Recognizing specific characteristics of nonspecific low back pain. Clin Orthop Relat Res. 1987. April;217:266-80. - PubMed
-
- Sembrano JN, Polly DW., Jr How often is low back pain not coming from the back? Spine (Phila Pa 1976). 2009. January 1;34(1):E27-32. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
