

Arterial carboxyhaemoglobin levels in children admitted to PICU: A retrospective observational study
- PMID: 30845230
- PMCID: PMC6405068
- DOI: 10.1371/journal.pone.0209452
Arterial carboxyhaemoglobin levels in children admitted to PICU: A retrospective observational study
Abstract
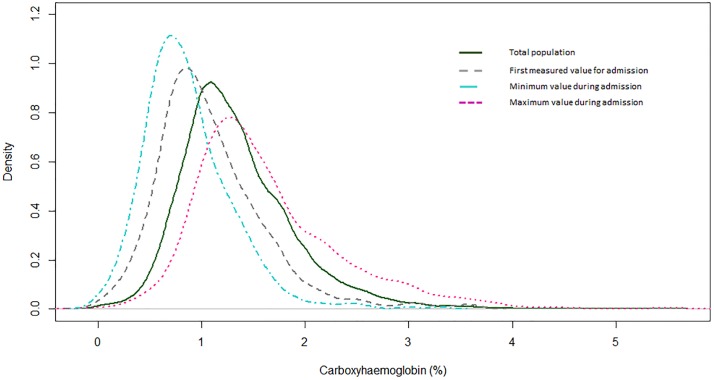
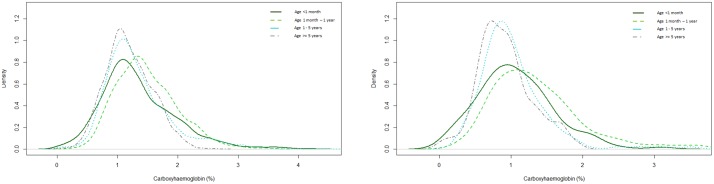
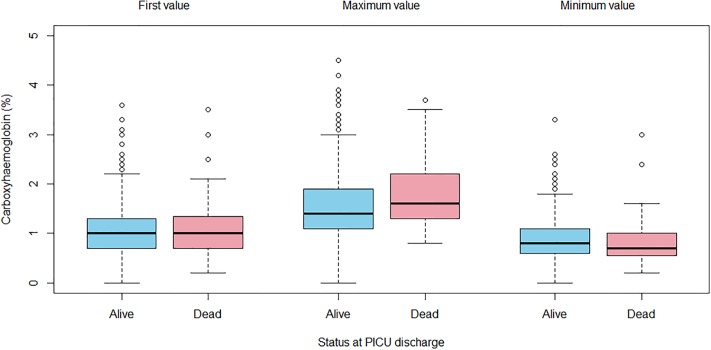
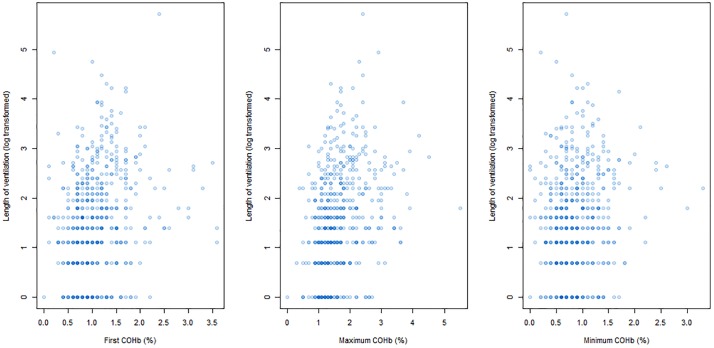
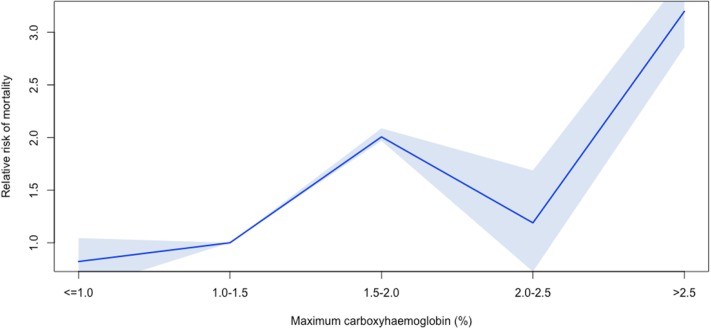
While carbon monoxide (CO) is considered toxic, low levels of endogenously produced CO are protective against cellular injury induced by oxidative stress. Carboxyhaemoglobin (COHb) levels have been associated with outcomes in critically ill adults. We aimed to describe the distribution of carboxyhaemoglobin in critically ill children and the relationship of these levels with clinical outcomes. This retrospective observational study was conducted at a large tertiary paediatric intensive care unit (PICU). We included all children admitted to the PICU over a two-year period who underwent arterial blood gas analysis. We measured the following: (i) Population and age-related differences in COHb distribution; (ii) Change in COHb over the first week of admission using a multi-level linear regression analysis; (iii) Uni- and multivariable relationships between COHb and length of ventilation and PICU survival. Arterial COHb levels were available for 559/2029 admissions. The median COHb level was 1.20% (IQR 1.00-1.60%). Younger children had significantly higher COHb levels (p-value <2 x 10-16). Maximum Carboxyhaemoglobin was associated with survival 1.67 (95% CI: 1.01-2.57; p-value = 0.02) and length of ventilation (OR 5.20, 95% CI: 3.07-7.30; p-value = 1.8 x 10-6) following multi-variable analysis. First measured and minimum COHb values were weakly associated with length of ventilation, but not survival. In conclusion, children have increased COHb levels in critical illness, which are greater in younger children. Higher COHb levels are associated with longer length of ventilation and death in PICU. This may reflect increased oxidative stress in these children.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
