

Complications from percutaneous microwave ablation of liver tumours: a pictorial review
- PMID: 30845823
- PMCID: PMC6636263
- DOI: 10.1259/bjr.20180864
Complications from percutaneous microwave ablation of liver tumours: a pictorial review
Abstract
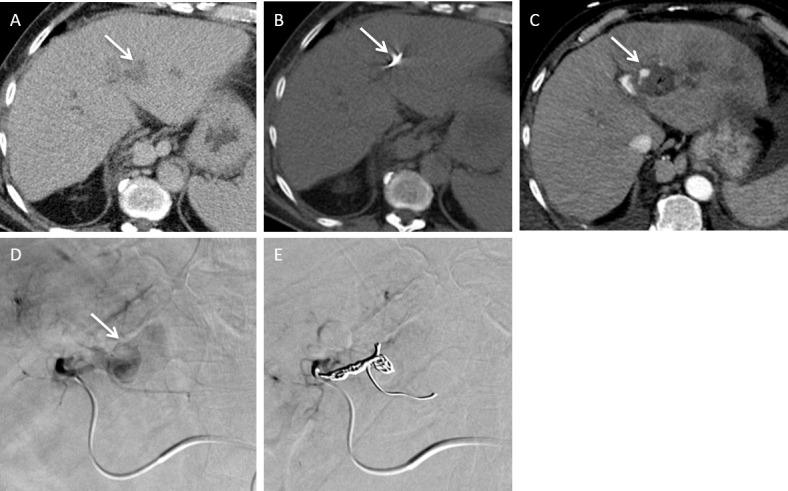
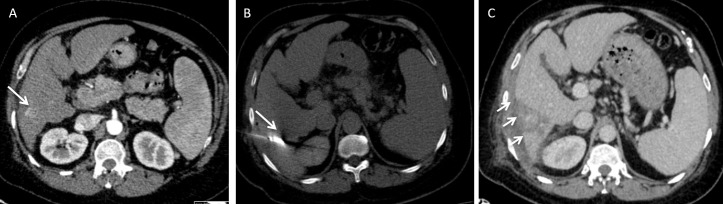
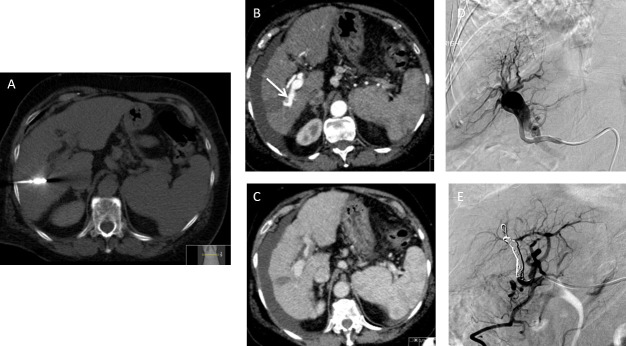
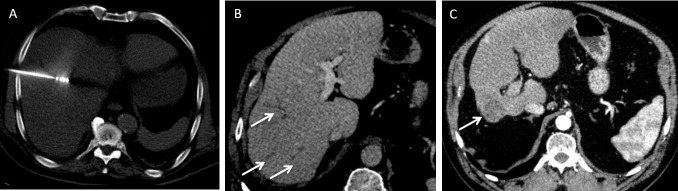
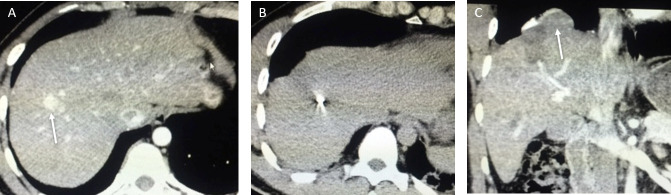
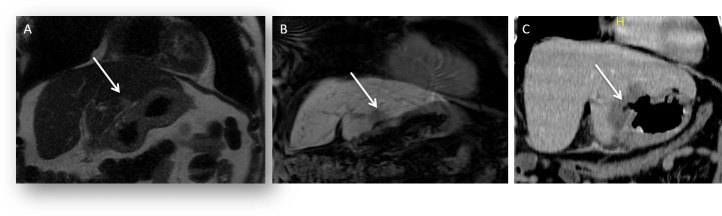
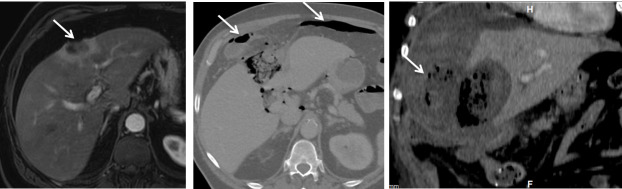
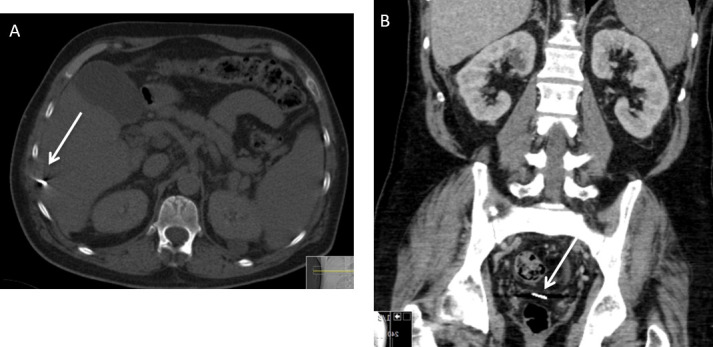
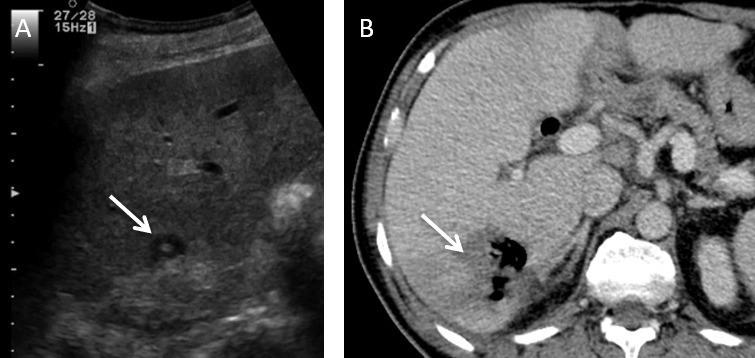
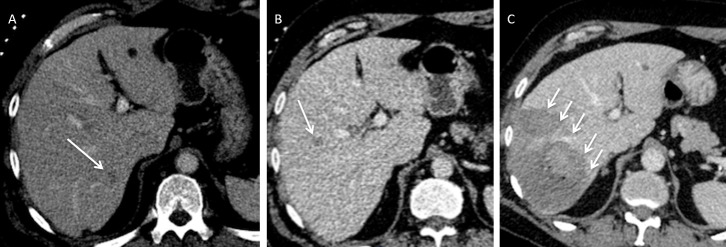
Percutaneous microwave ablation of liver tumours is a well-established technique that has been proven to be effective in the curative and palliative treatment of small volume primary and secondary liver tumours. Microwave ablation is designed to achieve larger areas of necrosis compared to radiofrequency ablation and has a good safety profile among liver tumour treatments. Mortality is unreported and major complications are rare. Knowledge of potential complications is essential for interventional radiologists performing liver ablation in order to reduce patient morbidity. The aim of this review is to illustrate major complications post microwave ablation in a pictorial format as well as a discussion on how best to avoid these complications.
Figures
References
-
- Ogata Y , Uchida S , Hisaka T , Horiuchi H , Mori S , Ishibashi N , et al. . Intraoperative thermal ablation therapy for small colorectal metastases to the liver . Hepatogastroenterology 2008. ; 55 ( 82–83 ): 550 – 6 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
