

Characteristics, Outcomes, and Treatment of Heart Failure With Improved Ejection Fraction
- PMID: 30845873
- PMCID: PMC6475046
- DOI: 10.1161/JAHA.118.011077
Characteristics, Outcomes, and Treatment of Heart Failure With Improved Ejection Fraction
Abstract
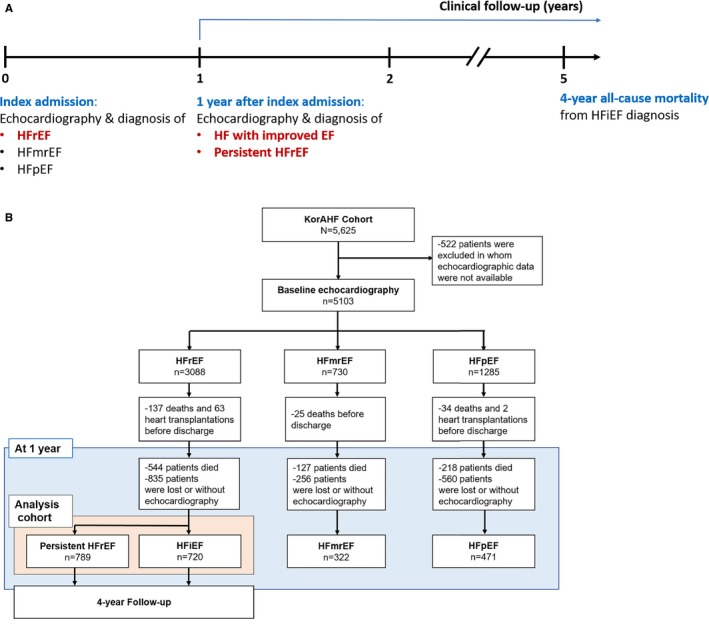
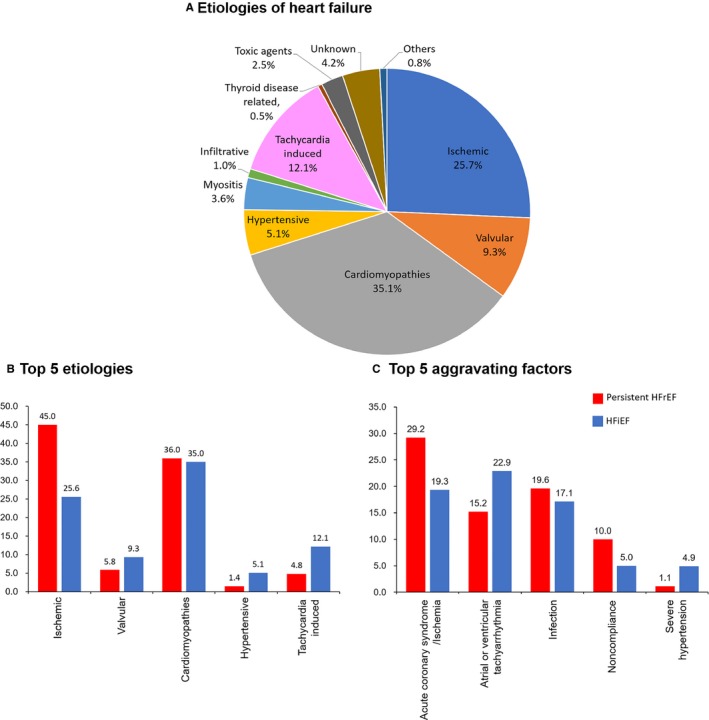
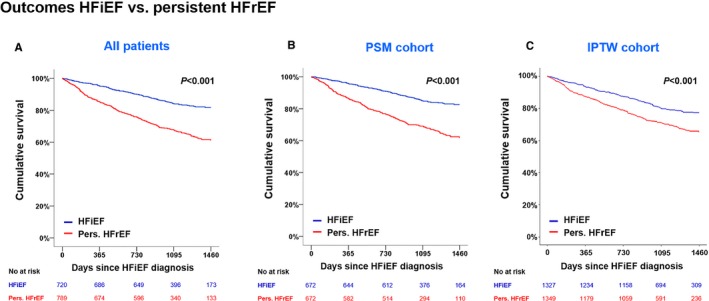
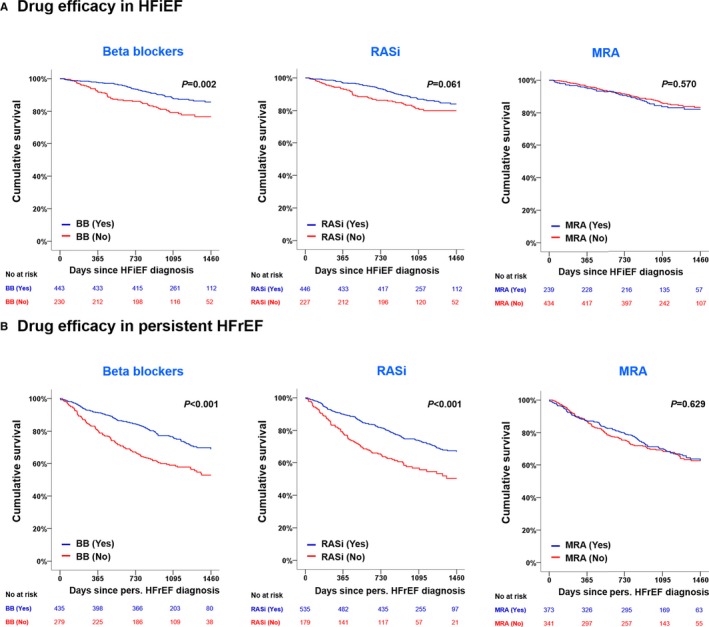
Background Many patients with heart failure ( HF ) with reduced ejection fraction ( HF r EF ) experience improvement or recovery of left ventricular ejection fraction ( LVEF ). Data on clinical characteristics, outcomes, and medical therapy in patients with HF with improved ejection fraction (HFiEF) are scarce. Methods and Results Of 5625 consecutive patients hospitalized for acute HF in the KorAHF (Registry [Prospective Cohort] for Heart Failure in Korea) study, 5103 patients had baseline echocardiography and 2302 patients had follow-up echocardiography at 12 months. HF phenotypes were defined as persistent HF r EF ( LVEF ≤40% at baseline and at 1-year follow-up), HF i EF ( LVEF ≤40% at baseline and improved up to 40% at 1-year follow-up), HF with midrange ejection fraction (LVEF between 40% and <50%), and HF with preserved ejection fraction ( LVEF ≥50%). The primary outcome was 4-year all-cause mortality from the time of HF i EF diagnosis. Among 1509 HF r EF patients who had echocardiography 1 year after index hospitalization, 720 (31.3%) were diagnosed as having HF i EF . Younger age, female sex, de novo HF , hypertension, atrial fibrillation, and β-blocker use were positive predictors and diabetes mellitus and ischemic heart disease were negative predictors of HF i EF . During 4-year follow-up, patients with HF i EF showed lower mortality than those with persistent HF r EF in univariate, multivariate, and propensity-score-matched analyses. β-Blockers, but not renin-angiotensin system inhibitors or mineralocorticoid receptor antagonists, were associated with a reduced all-cause mortality risk (hazard ratio: 0.59; 95% CI , 0.40-0.87; P=0.007). Benefits for outcome seemed similar among patients receiving low- or high-dose β-blockers (log-rank, P=0.304). Conclusions HF i EF is a distinct HF phenotype with better clinical outcomes than other phenotypes. The use of β-blockers may be beneficial for these patients. Clinical Trial Registration URL : https://www.clinicaltrials.gov . Unique identifier: NCT01389843.
Keywords: heart failure; improved ejection fraction; mortality; β‐blockers.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, Gonzalez‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; ESC Scientific Document Group . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. - PubMed
-
- Hogg K, McMurray J. Neurohumoral pathways in heart failure with preserved systolic function. Prog Cardiovasc Dis. 2005;47:357–366. - PubMed
-
- Kalogeropoulos AP, Fonarow GC, Georgiopoulou V, Burkman G, Siwamogsatham S, Patel A, Li S, Papadimitriou L, Butler J. Characteristics and outcomes of adult outpatients with heart failure and improved or recovered ejection fraction. JAMA Cardiol. 2016;1:510–518. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL; American College of Cardiology Foundation, American Heart Association Task Force on Practice Guidelines . 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:1810–1852. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
