

An open-label prospective study of the real-life use of onabotulinumtoxinA for the treatment of chronic migraine: the REPOSE study
- PMID: 30845917
- PMCID: PMC6734221
- DOI: 10.1186/s10194-019-0976-1
An open-label prospective study of the real-life use of onabotulinumtoxinA for the treatment of chronic migraine: the REPOSE study
Abstract
Background: The PREEMPT Studies established onabotulinumtoxinA as preventive treatment for adults with chronic migraine (CM). The purpose of the REal-life use of botulinum toxin for the symptomatic treatment of adults with chronic migraine, measuring healthcare resource utilisation, and Patient-reported OutcomeS observed in practice (REPOSE) Study was to observe real-life, long-term (24-month) use of onabotulinumtoxinA in adults with CM and report on the utilisation, effectiveness, safety, and tolerability.
Methods: The REPOSE Study was a European, open-label, multicentre, prospective, noninterventional study. Patients received onabotulinumtoxinA approximately every 12 weeks according to their physician's usual practice, guided by the summary of product characteristics (SPC). Patients were observed for 24 months after initiating onabotulinumtoxinA treatment. Outcome measures were collected at baseline and all administration visits and included onabotulinumtoxinA injection practices, headache-day frequency, Migraine-Specific Quality-of-Life Questionnaire (MSQ), EuroQol 5-Dimension Questionnaire (EQ-5D), and adverse drug reactions (ADRs) to evaluate safety/tolerability.
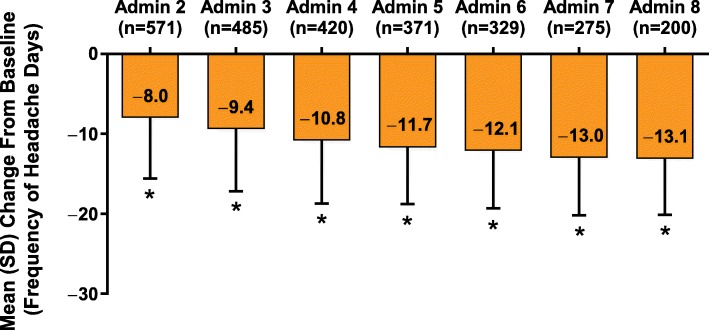
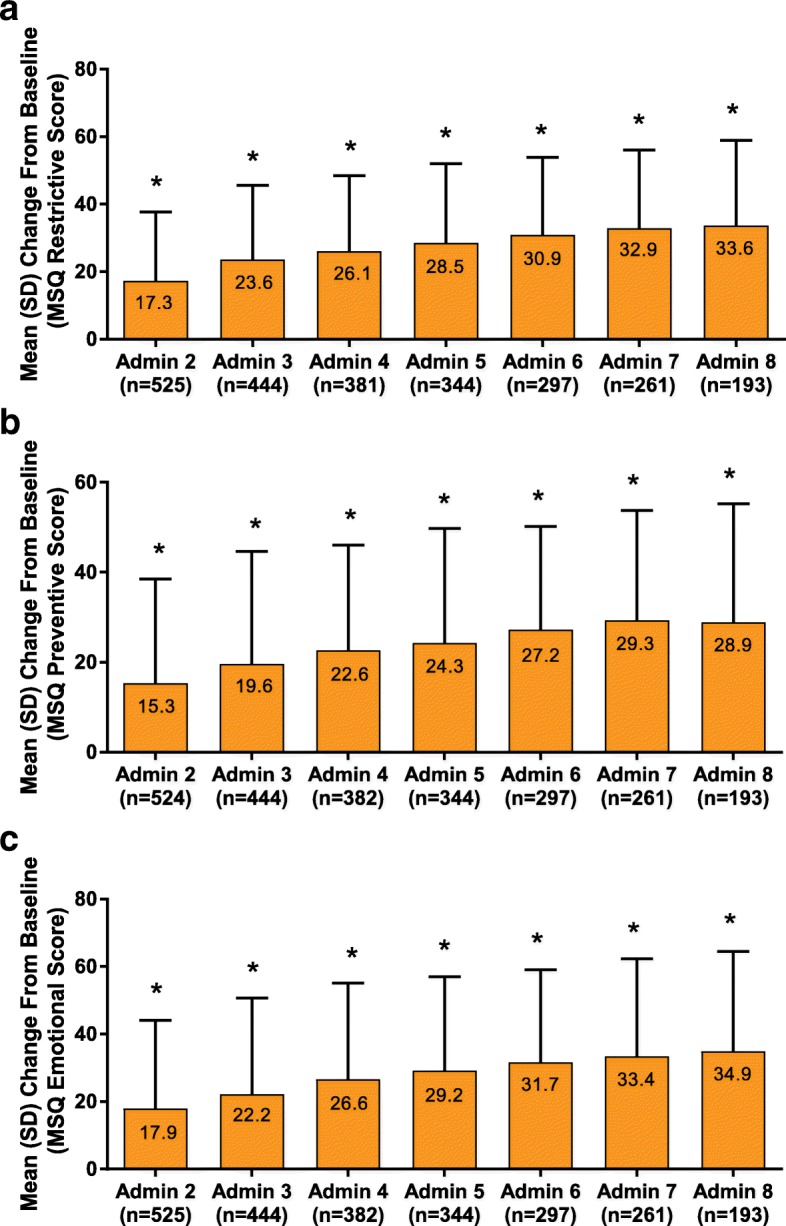
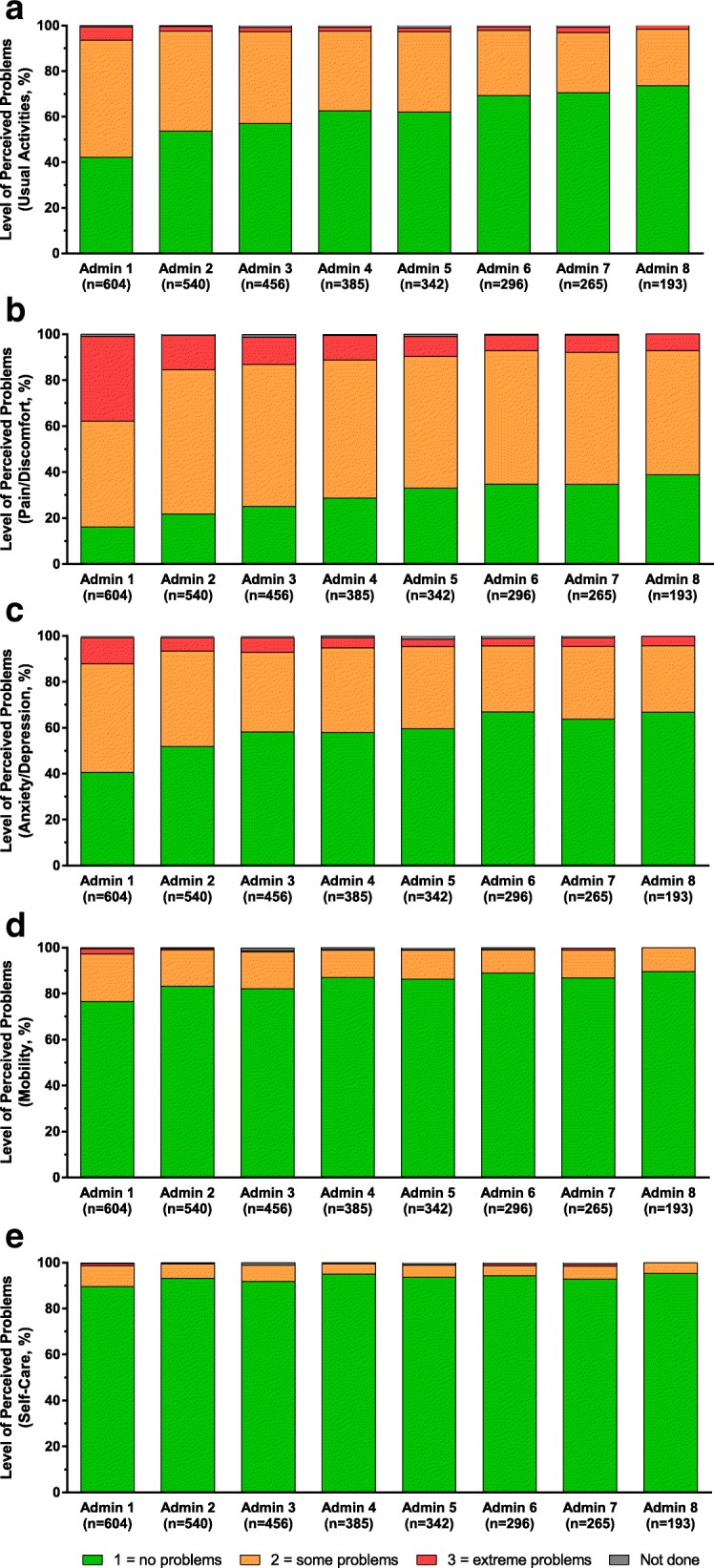
Results: Of 641 patients enrolled, 633 received ≥1 dose of onabotulinumtoxinA for a total of 3499 treatment sessions. At baseline, mean (SD) age was 45.4 (11.7) years; patients were predominantly women (85.3%). Injection practices closely followed the SPC in mean dosage (155.1 U) and injection sites per session (31.4), with the exception of a prolongation of the recommended 12-week dosing interval, with 79.1% of patients receiving ≥1 treatment session that was > 13 weeks after the previous treatment session. Headache-day frequency was reduced from a baseline mean (SD) of 20.6 (5.4) to 7.4 (6.6) days at administration visit 8 (P < 0.001). Each MSQ domain (restrictive, preventive, and emotional) was significantly reduced from baseline through each administration visit (P < 0.001). The median EQ-5D total and health state scores were significantly improved from baseline through each administration visit (P < 0.001). Overall, 18.3% of patients reported an ADR; most were mild to moderate intensity, with only 1.3% of patients reporting a serious ADR. Eyelid ptosis (5.4%), neck pain (2.8%), and musculoskeletal stiffness (2.7%) were the most frequently reported.
Conclusions: Long-term, real-world preventive treatment of CM with onabotulinumtoxinA showed effectiveness with a sustained reduction in headache-day frequency and significant improvement in quality-of-life measures. ADRs were mild to moderate, with no new safety concerns identified.
Trial registration: Trial registration number: NCT01686581. Name of registry: ClinicalTrials.gov. URL of registry: https://clinicaltrials.gov/ct2/show/NCT01686581 . Date of retrospective registration: September 18, 2012. Date of enrolment of first patient: July 23, 2012.
Keywords: Chronic migraine; Clinical setting; Effectiveness; Long-term; OnabotulinumtoxinA; Real world; Safety.
Conflict of interest statement
Fayyaz Ahmed declares that he has received honorarium for consultancy and lecturing from Allergan, Eneura, ElectroCore, and Novartis, which is paid to the British Association for the Study of Headache and the Migraine Trust. Charly Gaul is the director of the Migraine and Headache Clinic Königstein. He has received honoraria from Allergan, Ratiopharm, Boehringer Ingelheim, Lilly, Novartis, Desitin Arzneimittel, Cerbotec, Bayer Vital, Hormosan, ElectroCore und Grünenthal, Reckitt Benckiser, and Teva. Dr. Gaul has no ownership interests and does not own any pharmaceutical company stocks. Juan Carlos García-Moncó declares he has consulted for Allergan. Katherine Sommer is an employee of Allergan plc (Marlow, Buckinghamshire, UK) and holds stock in the company. Paolo Martelletti declares that he has received research funds or advisory board honoraria from Allergan, Amgen, ElectroCore, Elytra Pharma, Teva, Novartis, and Bayer; travel reimbursement from Springer Nature and EMA; and royalties from Springer.
Figures

Similar articles
-
Real-life use of onabotulinumtoxinA for symptom relief in patients with chronic migraine: REPOSE study methodology and baseline data.J Headache Pain. 2017 Sep 6;18(1):93. doi: 10.1186/s10194-017-0802-6. J Headache Pain. 2017. PMID: 28879545 Free PMC article.
-
Real-World Safety and Efficacy of 156 U - 195 U OnabotulinumtoxinA in Adults With Chronic Migraine: Results From the REPOSE Study.BMC Neurol. 2025 May 6;25(1):197. doi: 10.1186/s12883-025-04087-7. BMC Neurol. 2025. PMID: 40329224 Free PMC article.
-
Real-life use of onabotulinumtoxinA reduces healthcare resource utilization in individuals with chronic migraine: the REPOSE study.J Headache Pain. 2021 Jun 2;22(1):50. doi: 10.1186/s10194-021-01260-4. J Headache Pain. 2021. PMID: 34078259 Free PMC article.
-
OnabotulinumtoxinA injection in the treatment of chronic migraine.Prog Brain Res. 2020;255:171-206. doi: 10.1016/bs.pbr.2020.05.013. Epub 2020 Jun 30. Prog Brain Res. 2020. PMID: 33008506 Review.
-
Development of onabotulinumtoxinA for chronic migraine.Ann N Y Acad Sci. 2014 Nov;1329:67-80. doi: 10.1111/nyas.12488. Epub 2014 Aug 18. Ann N Y Acad Sci. 2014. PMID: 25399521 Review.
Cited by
-
OnabotulinumtoxinA: Still the Present for Chronic Migraine.Toxins (Basel). 2023 Jan 10;15(1):59. doi: 10.3390/toxins15010059. Toxins (Basel). 2023. PMID: 36668879 Free PMC article. Review.
-
Real-World Evidence for the Safety and Efficacy of CGRP Monoclonal Antibody Therapy Added to OnabotulinumtoxinA Treatment for Migraine Prevention in Adult Patients With Chronic Migraine.Front Neurol. 2022 Jan 6;12:788159. doi: 10.3389/fneur.2021.788159. eCollection 2021. Front Neurol. 2022. PMID: 35069416 Free PMC article.
-
Headache for ophthalmologists: current advances in headache understanding and management.Eye (Lond). 2021 Jun;35(6):1574-1586. doi: 10.1038/s41433-021-01421-4. Epub 2021 Feb 12. Eye (Lond). 2021. PMID: 33580185 Free PMC article. Review.
-
Real-World Evidence of the Safety and Effectiveness of Atogepant Added to OnabotulinumtoxinA for the Preventive Treatment of Chronic Migraine: A Retrospective Chart Review.Pain Ther. 2024 Dec;13(6):1571-1587. doi: 10.1007/s40122-024-00649-8. Epub 2024 Sep 17. Pain Ther. 2024. PMID: 39287781 Free PMC article.
-
The effectiveness and predictors influencing the outcome of onabotulinumtoxinA treatment in chronic migraine: understanding from diverse patient profiles in a single session.Front Neurol. 2024 Jun 19;15:1417303. doi: 10.3389/fneur.2024.1417303. eCollection 2024. Front Neurol. 2024. PMID: 38962481 Free PMC article.
References
-
- Schwedt TJ. Chronic migraine. BMJ (Clinical research ed) 2014;348:g1416. - PubMed
-
- Headache Classification Committee of the International Headache Society The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38:1–211. - PubMed
-
- Lanteri-Minet M, Duru G, Mudge M, Cottrell S. Quality of life impairment, disability and economic burden associated with chronic daily headache, focusing on chronic migraine with or without medication overuse: a systematic review. Cephalalgia. 2011;31:837–850. doi: 10.1177/0333102411398400. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
