

Treatment delay in status epilepticus - more effective prehospital symptom recognition warranted
- PMID: 30845979
- PMCID: PMC6407251
- DOI: 10.1186/s13049-019-0605-7
Treatment delay in status epilepticus - more effective prehospital symptom recognition warranted
Abstract
Background: The outcome of status epilepticus (SE) can be improved by facilitating early recognition and treatment with antiepileptic drugs. The purpose of this study was to analyze the treatment delay of SE in a prospectively recruited patient cohort. Improvements to the treatment process are suggested.
Methods: Consecutive adult patients with SE were recruited in the emergency department of Kuopio University Hospital (KUH) between March 23 and December 31, 2015. SE was defined as a prolonged (> 5 min) epileptic seizure or recurrent tonic-clonic seizures (≥ 3 seizures within any 24 h). Diagnostic and treatment delays and the features of SE were subject to statistical analysis.
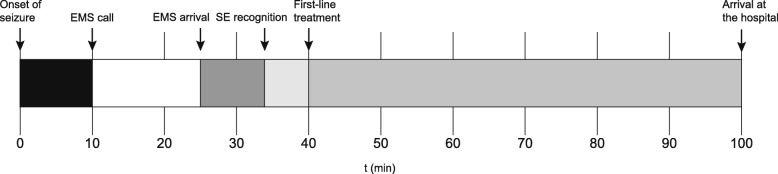
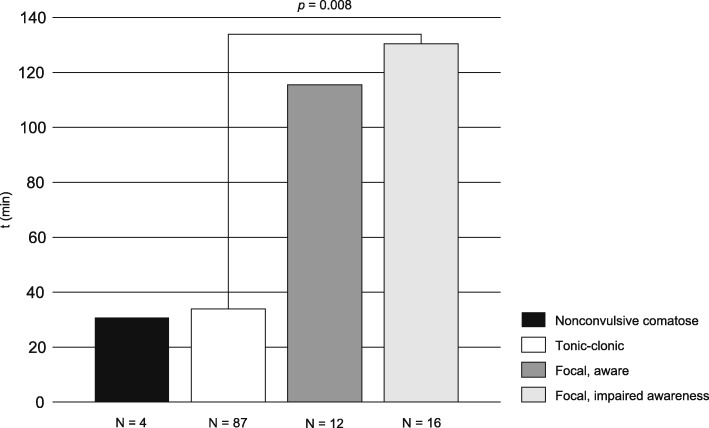
Results: We recorded 151 cases of SE during the study period. First-line treatment was initiated outside of hospital in 79 cases (52.3%), with a significantly shorter median delay compared to intrahospital initiation (28 min vs. 2 h 5 min, p < 0.001). Forty-six episodes of SE (30.5%) were not recognized during the prehospital phase. The median delay in recognition of tonic-clonic SE (23 min) was significantly shorter than in focal aware (2 h 0 min, p = 0.045) or focal impaired awareness SE (2 h 25 min, p < 0.001). Second-line treatment was used in 91 cases (60.3%), with a median delay of 2 h 42 min. Anesthesia was used in seven cases (4.6%) with refractory SE, with a median delay of 6 h 40 min.
Conclusions: SE is often not recognized during the prehospital phase of treatment, which delays the initiation of first-line treatment. Intrahospital delay could be reduced by streamlining patient transition between the three lines of treatment.
Keywords: Delay; Emergency; Paramedic; Seizure; Status epilepticus; Treatment.
Conflict of interest statement
Ethics approval and consent to participate
The Committee on Research Ethics of North Savo Hospital District approved the study design. The use of medical records was authorized by the hospital district in accordance with Finnish legislation. Informed consent was waived because of the non-interventional nature of the study. Subject rights and confidentiality were protected by using anonymous clinical data in all analyses.
Consent for publication
Not applicable.
Competing interests
JS has received grants from the Finnish Epilepsy Research Foundation and the Maire Taponen Foundation and institutional funding from the Finnish State Research Funding via Neurocenter, Kuopio University Hospital. AMK has received a grant from the Finnish Cultural Foundation and speaker’s honoraria from Orion, Boehringer Ingelheim, MSD, BMS and a travel grant from Sanofi. HH has received speaker’s honoraria from Orion and Boehringer Ingelheim and honoraria for the membership of advisory board from MSD. RK has received grants from the Academy of Finland and the Saastamoinen Foundation, speaker’s honoraria from Eisai, UCV and Orion and honoraria for the membership of advisory board from Eisai, Fennomedical, GW Pharmaceuticals, Sage Therapeutics, Takeda and UCB.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
