

CT and Multimodal MR Imaging Features of Embryonal Tumors with Multilayered Rosettes in Children
- PMID: 30846437
- PMCID: PMC7048518
- DOI: 10.3174/ajnr.A6001
CT and Multimodal MR Imaging Features of Embryonal Tumors with Multilayered Rosettes in Children
Abstract
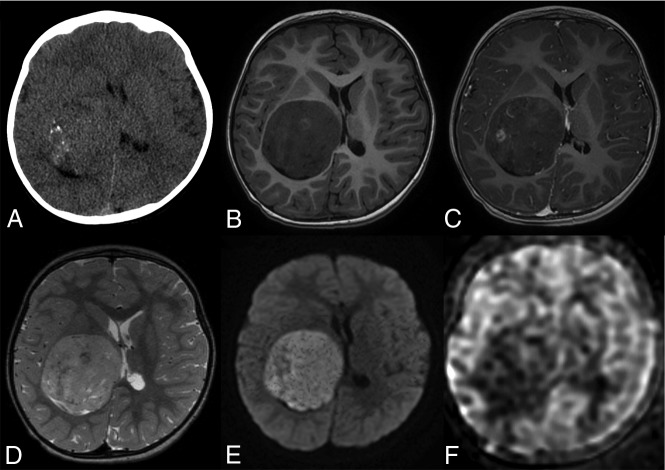
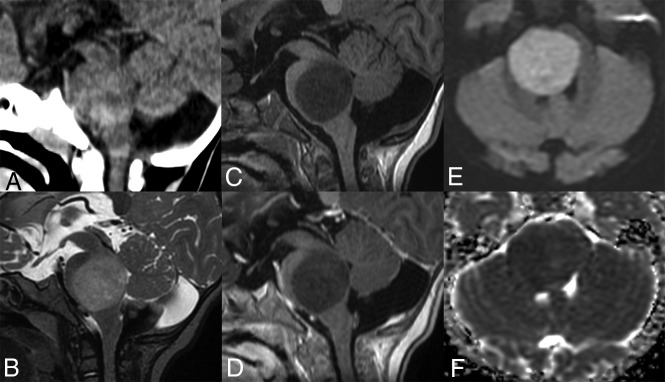
Background and purpose: Embryonal tumors with multilayered rosettes, C19MC-altered, are brain tumors occurring in young children, which were clearly defined in the 2016 World Health Organization classification of central nervous system neoplasms. Our objective was to describe the multimodal imaging characteristics of this new entity.
Materials and methods: We performed a retrospective monocentric review of embryonal brain tumors and looked for embryonal tumors with multilayered rosettes with confirmed C19MC alteration. We gathered morphologic imaging data, as well as DWI and PWI data (using arterial spin-labeling and DSC).
Results: We included 16 patients with a median age of 2 years 8 months. Tumors were both supratentorial (56%, 9/16) and infratentorial (44%, 7/16). Tumors were large (median diameter, 59 mm; interquartile range, 48-71 mm), with absent (75%, 12/16) or minimal (25%, 4/16) peritumoral edema. Enhancement was absent (20%, 3/15) or weak (73%, 11/15), whereas intratumoral macrovessels were frequently seen (94%, 15/16) and calcifications were present in 67% (10/15). Diffusion was always restricted, with a minimal ADC of 520 mm2/s (interquartile range, 495-540 mm2/s). Cerebral blood flow using arterial spin-labeling was low, with a maximal CBF of 43 mL/min/100 g (interquartile range, 33-55 mL/min/100 g 5). When available (3 patients), relative cerebral blood volume using DSC was high (range, 3.5-5.8).
Conclusions: Embryonal tumors with multilayered rosettes, C19MC-altered, have characteristic imaging features that could help in the diagnosis of this rare tumor in young children.
© 2019 by American Journal of Neuroradiology.
Figures


References
-
- Korshunov A, Sturm D, Ryzhova M, et al. Embryonal tumor with abundant neuropil and true rosettes (ETANTR), ependymoblastoma, and medulloepithelioma share molecular similarity and comprise a single clinicopathological entity. Acta Neuropathol (Berl) 2014;128:279–89 10.1007/s00401-013-1228-0 - DOI - PMC - PubMed
-
- Ryzhova MV, Zheludkova OG, Ozerov SS, et al. A new entity in WHO classification of tumors of the central nervous system–embryonic tumor with abundant neuropil and true rosettes: case report and review of literature. Zh Vopr Neirokhir Im N N Burdenko 2011;75:25–33 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical