

Cervical Artificial Disc Replacement Versus Fusion for Cervical Degenerative Disc Disease: A Health Technology Assessment
- PMID: 30847009
- PMCID: PMC6394883
Cervical Artificial Disc Replacement Versus Fusion for Cervical Degenerative Disc Disease: A Health Technology Assessment
Abstract
Background: Cervical degenerative disc disease is a multifactorial condition that begins with deterioration of the intervertebral disc and results in further degeneration within the spine involving the facet joints and ligaments. This health technology assessment examined the effectiveness, safety, durability, and cost-effectiveness of cervical artificial disc replacement (C-ADR) versus fusion for treating cervical degenerative disc disease.
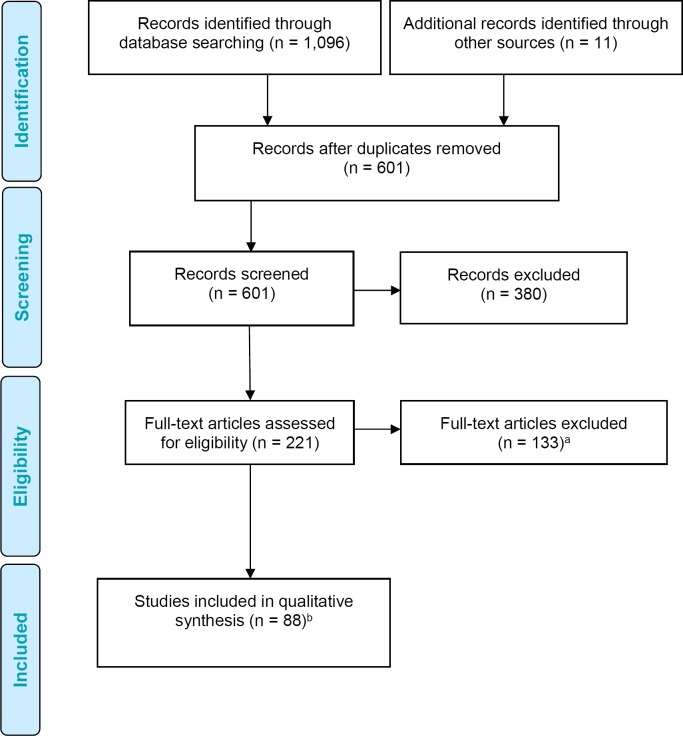
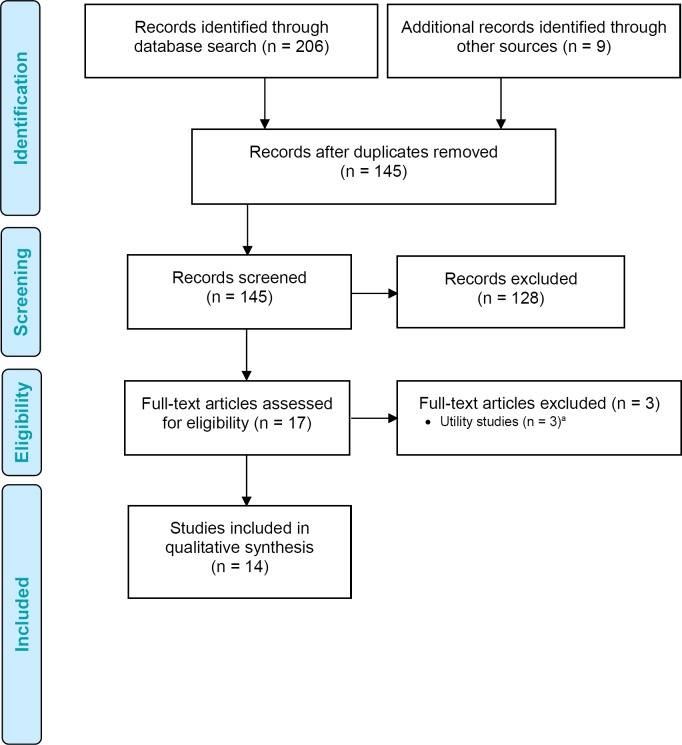
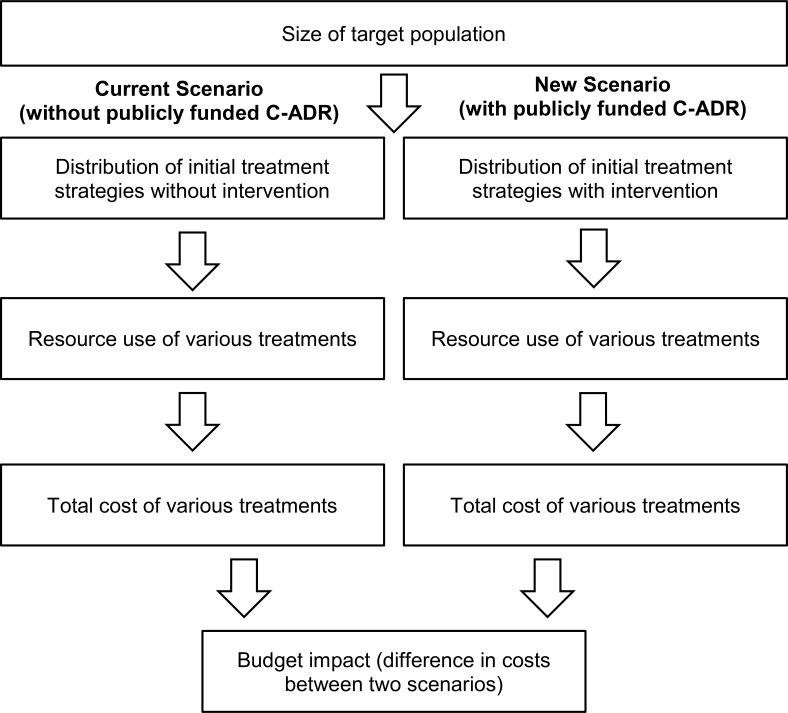
Methods: We performed a systematic literature search of the clinical evidence comparing C-ADR with fusion. We assessed the risk of bias in each study and the quality of the body of evidence according to the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Working Group criteria. We performed a systematic review of the economic literature and assessed the cost-effectiveness of C-ADR compared with fusion. We also estimated the budget impact of publicly funding C-ADR in Ontario over the next 5 years. To contextualize the potential value of C-ADR, we spoke with people with cervical degenerative disc disease.
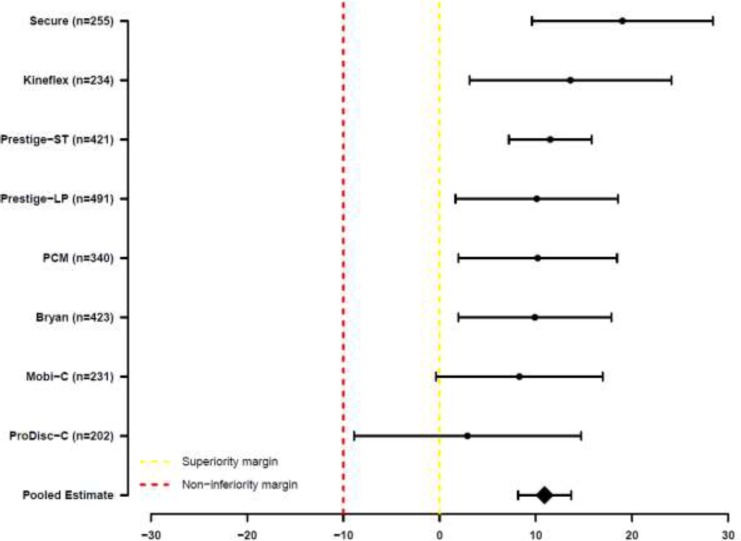
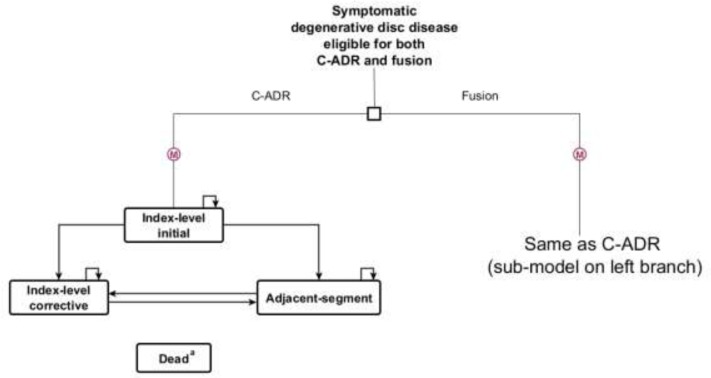
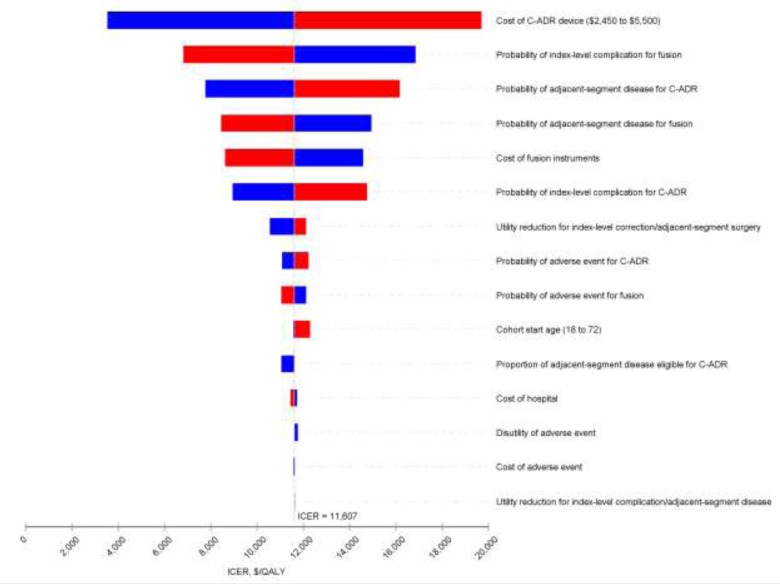
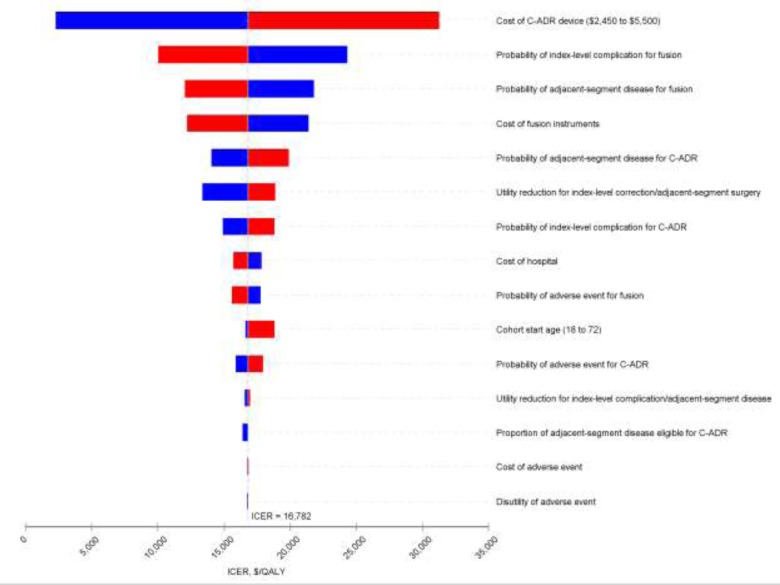
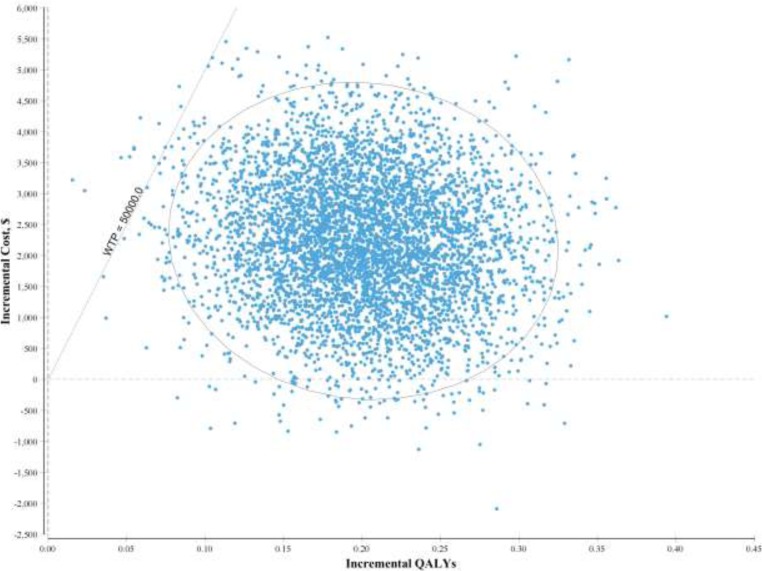
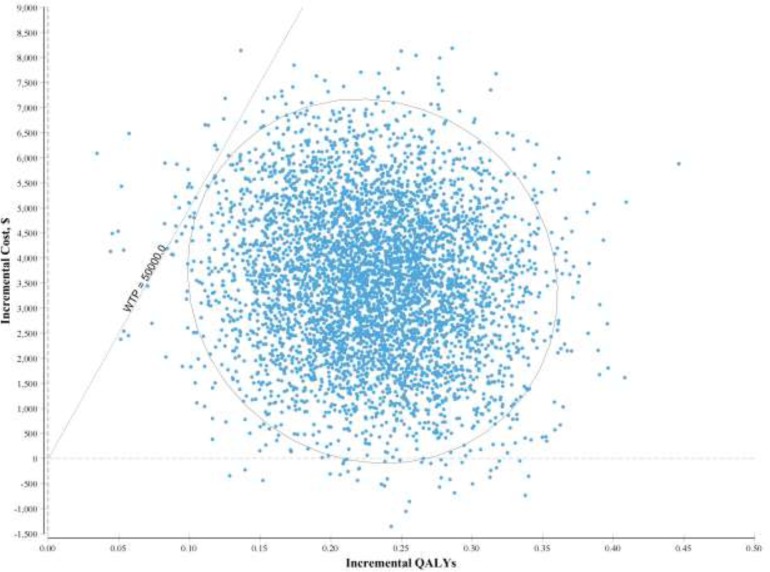
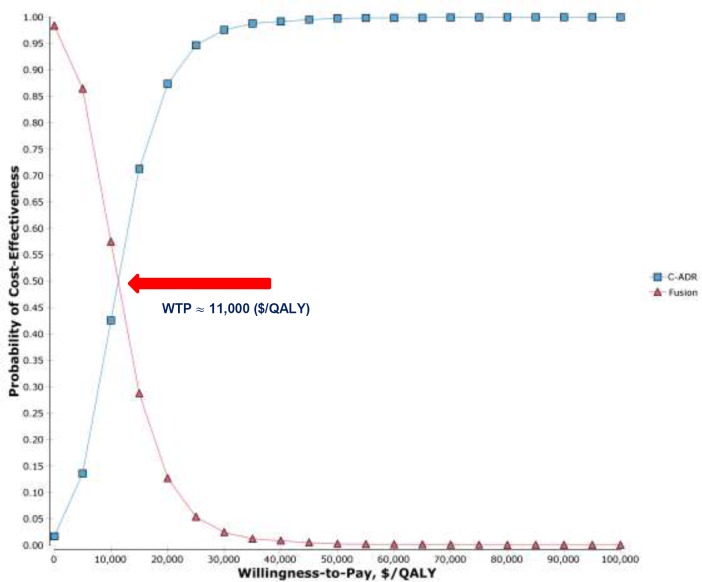
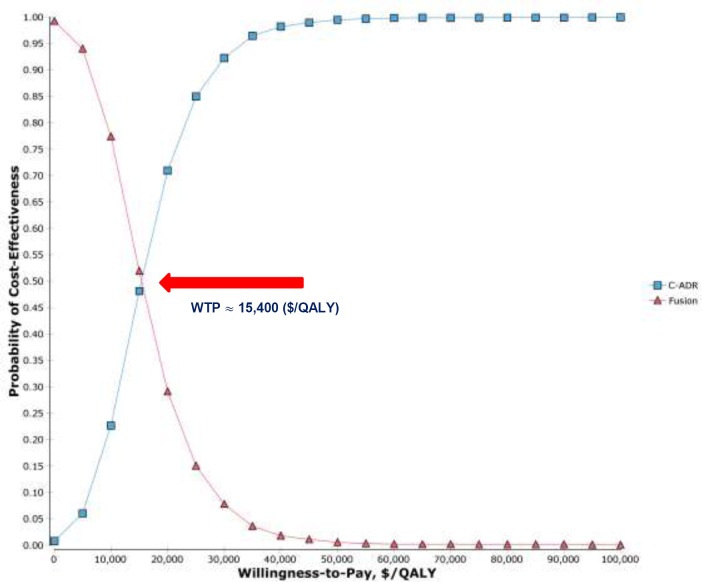
Results: Eight studies of C-ADR for one-level cervical degenerative disc disease and two studies of C-ADR for two-level disease satisfied the criterion of statistical noninferiority compared with fusion on the primary outcome of 2-year overall treatment success (GRADE: Moderate). In two studies of C-ADR for two-level disease, C-ADR was statistically superior to fusion surgery for the same primary outcome (GRADE: Moderate). C-ADR was also noninferior to fusion for perioperative outcomes (e.g., operative time, blood loss), patient satisfaction, and health-related quality of life (GRADE: Moderate). C-ADR was superior to fusion for recovery and return to work, had higher technical success, and had lower rates of re-operation at the index site (GRADE: Moderate). C-ADR also maintained motion at the index-treated cervical level (GRADE: Moderate), but evidence was insufficient to determine if adjacent-level surgery rates differed between C-ADR and fusion. Current evidence is also insufficient to determine the long-term durability of C-ADR.The primary economic analysis shows that C-ADR is likely to be cost-effective compared with fusion for both one-level ($11,607/quality-adjusted life-year [QALY]) and two-level ($16,782/QALY) degeneration. Various sensitivity and scenario analyses confirm the robustness of the results. The current uptake for one-level and two-level C-ADR in Ontario is about 8% of the total eligible. For one-level involvement, the estimated net budget impact increases from $7,243 (18 procedures) in the first year to $395,623 (196 procedures) in the fifth year following public funding, for a total budget impact over 5 years of $916,326. For two-level involvement, the corresponding values are $5,460 (7 procedures) in the first year and $283,689 (76 procedures) in the fifth year, for an estimated total budget impact of $705,628 over 5 years.People with cervical degenerative disc disease reported that symptoms of pain and numbness can have a negative impact on their quality of life. People with whom we spoke had tried a variety of treatments with minor success; surgery was perceived as the most effective and permanent solution. Those who had undergone C-ADR spoke positively of its impact on their quality of life and ability to move their neck after surgery. The limited availability of C-ADR in Ontario was viewed as a barrier to receiving this treatment.
Conclusions: For carefully selected patients with cervical degenerative disc disease, C-ADR provides patient-important and statistically significant reductions in pain and disability. Further, unlike fusion, C-ADR allows people to maintain relatively normal cervical spine motion.Compared with fusion, C-ADR appears to represent good value for money for adults with one-level cervical degenerative disc disease ($11,607/QALY) and for adults with two-level disease ($16,782/QALY). In Ontario, publicly funding C-ADR could result in total additional costs of $916,326 for one-level procedures and $705,628 for two-level procedures over the next 5 years.People with whom we spoke who had undergone C-ADR surgery spoke positively of its impact on their quality of life and ability to move their neck after surgery. The limited availability of C-ADR in Ontario was viewed as a barrier to receiving this treatment.
Figures
Similar articles
-
Artificial discs for lumbar and cervical degenerative disc disease -update: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(10):1-98. Epub 2006 Apr 1. Ont Health Technol Assess Ser. 2006. PMID: 23074480 Free PMC article.
-
Seven-year cost-effectiveness of ProDisc-C total disc replacement: results from investigational device exemption and post-approval studies.J Neurosurg Spine. 2016 May;24(5):760-8. doi: 10.3171/2015.10.SPINE15505. Epub 2016 Jan 29. J Neurosurg Spine. 2016. PMID: 26824587 Clinical Trial.
-
Transcatheter Aortic Valve Implantation in Patients With Severe Aortic Valve Stenosis at Low Surgical Risk: A Health Technology Assessment.Ont Health Technol Assess Ser. 2020 Nov 2;20(14):1-148. eCollection 2020. Ont Health Technol Assess Ser. 2020. PMID: 33240455 Free PMC article.
-
Multi-gene Pharmacogenomic Testing That Includes Decision-Support Tools to Guide Medication Selection for Major Depression: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(13):1-214. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484487 Free PMC article.
-
Internet-Delivered Cognitive Behavioural Therapy for Major Depression and Anxiety Disorders: A Health Technology Assessment.Ont Health Technol Assess Ser. 2019 Feb 19;19(6):1-199. eCollection 2019. Ont Health Technol Assess Ser. 2019. PMID: 30873251 Free PMC article.
Cited by
-
Qualitative and quantitative retrieval analysis of a ball-and-socket cervical disc replacement.N Am Spine Soc J. 2025 Jul 5;23:100768. doi: 10.1016/j.xnsj.2025.100768. eCollection 2025 Sep. N Am Spine Soc J. 2025. PMID: 40791669 Free PMC article.
-
Posterior intraprosthetic dislocation of cervical arthroplasty: illustrative case.J Neurosurg Case Lessons. 2021 Dec 6;2(23):CASE21500. doi: 10.3171/CASE21500. eCollection 2021 Dec 6. J Neurosurg Case Lessons. 2021. PMID: 36061081 Free PMC article.
-
Bibliometric and visualized analysis of the top 100 most-cited articles on anterior cervical surgery.EFORT Open Rev. 2021 Dec 10;6(12):1203-1213. doi: 10.1302/2058-5241.6.210074. EFORT Open Rev. 2021. PMID: 35726846 Free PMC article. Review.
-
Assessing the potential role of ChatGPT in spine surgery research.J Exp Orthop. 2024 Jun 13;11(3):e12057. doi: 10.1002/jeo2.12057. eCollection 2024 Jul. J Exp Orthop. 2024. PMID: 38873173 Free PMC article.
References
-
- Prescher A. Anatomy and pathology of the aging spine. Eur J Radiol. 1998;27(3):181–95. - PubMed
-
- Edwards CC, 2nd, Riew KD, Anderson PA, Hilibrand AS, Vaccaro AF. Cervical myelopathy. Current diagnostic and treatment strategies. Spine J. 2003;3(1):68–81. - PubMed
-
- Radhakrishnan K, Litchy WJ, O'Fallon WM, Kurland LT. Epidemiology of cervical radiculopathy: a population-based study from Rochester, Minnesota, 1976. through 1990. Brain. 1994;117:325–35. - PubMed
-
- Moore AP, Blumhardt LD. A prospective survey of the causes of non-traumatic spastic paraparesis and tetraparesis in 585 patients. Spinal Cord. 1997;35(6):361–7. - PubMed
-
- Nouri A, Tetreault L, Singh A, Karadimas SK, Fehlings MG. Degenerative cervical myelopathy: epidemiology, genetics, and pathogenesis. Spine (Phila Pa 1976). 2015;40(12):E675–93. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials